All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Editorial theme │ Induction therapy for AML: Recent progress
Efforts to improve induction therapy outcomes in patients with acute myeloid leukemia (AML) have proven difficult. Broader understanding of the molecular pathophysiology of the disease has provided opportunities to develop targeted therapies for patients who are ineligible for intensive chemotherapy, to ultimately improve survival outcomes when added to intensive chemotherapeutic backbones.
In this editorial theme on induction therapy, we summarize recent data investigating targeted agents for intensive induction therapy, and real-world survival outcomes for patients ineligible for intensive chemotherapy.
Intensive chemotherapy
The therapeutic mainstay for intensive chemotherapy in AML is the ‘3 + 7 regimen’ (3 days of daunorubicin + 7 days of cytarabine) with variations to the chemotherapeutic backbone.1 Recently, improved understanding of genetic and cytogenetic abnormalities that may impair response to chemotherapy alone has led to the development and approval of targeted therapies.
FLT3 inhibitors
For patients with internal tandem duplications (ITD) or tyrosine kinase domain (TKD) point mutations of the fms-related tyrosine kinase 3 gene (FLT3), addition of the multitargeted kinase inhibitor midostaurin to standard chemotherapy has shown prolonged survival.2 The pivotal phase III RATIFY trial (NCT00651261) demonstrated significant improvements in median overall survival (OS) and event-free survival (EFS) with the addition of midostaurin to standard chemotherapeutic backbone (induction therapy with daunorubicin plus cytarabine and consolidation therapy with high-dose cytarabine). The benefit of midostaurin was consistent across all FLT3 subtypes. Further research is ongoing to evaluate the efficacy of more specific FLT3 inhibitors, such as quizartinib and gilteritinib, or another nonspecific FLT3 inhibitor, sorafenib.2
Gemtuzumab ozogamicin
Gemtuzumab ozogamicin (GO), an anti-CD33 antibody-drug conjugate, was approved in 2017 by the U.S. Food and Drug Administration (FDA) for adult patients with newly diagnosed de novo CD33-positive AML. The best way to use GO in induction therapy is uncertain, however. Recent data indicate that patients with newly diagnosed AML benefit from fractionated doses of GO when combined with cladribine, high-dose cytarabine, granulocyte colony-stimulating factor (G-CSF) and mitoxantrone (CLAG-M).3
IDH1 and IDH2 inhibitors
In patients with newly diagnosed AML, the isocitrate dehydrogenase 1 (IDH1) inhibitor ivosidenib, and IDH2 inhibitor enasidenib, have demonstrated complete response (CR) rates of >70% in a phase I trial when combined with intensive induction and consolidation chemotherapy. IDH inhibitors were well tolerated, and no deaths related to treatment were observed.4
Venetoclax
The benefit of the BCL-2 inhibitor venetoclax has been investigated with intensive chemotherapy regimens. For example, a recent phase II single arm study demonstrated durable CR rates in younger patients (<65 years old) with newly-diagnosed AML, treated with venetoclax in combination with a high intensive chemotherapy regimen of cladribine with higher dose cytarabine and idarubicin.5
Eprenetapopt (APR-246)
TP53 mutations are consistently associated with poor prognosis and reduced OS. Eprenetapopt is a p53 reactivator with orphan drug designation by the FDA in TP53-mutant myelodysplastic syndromes (MDS). In a recent phase II trial, eprenetapopt with azacitidine demonstrated that median OS was significantly improved in a combined cohort of patients with TP53-mutant MDS or oligoblastic AML, with a median OS of 11.8 months in all patients.6
Overall, there has been a rapid expansion of clinical trials for targeted agents in newly diagnosed AML in recent years; combinations of targeted therapies with intensive chemotherapy or alone are still to be explored.
Non-intensive induction therapy
The use of non-intensive induction therapy, namely, low-dose cytarabine (LDAC), hypomethylating agents (HMAs), or best supportive care (BSC), is the standard for patients unfit for intensive chemotherapy. Clinical trial data have demonstrated consistent poor OS across these therapies in older patients with AML unable to tolerate intensive chemotherapy. A recent registry analysis provided real-world evidence that patients receiving intensive induction have greater remission rates and better OS compared with patients who receive non-intensive induction.7
Further analysis of non-intensive chemotherapy outcomes was presented in a large noninterventional retrospective study at the 62nd American Society of Hematology (ASH) Annual Meeting and Exposition (ASH 2020), including 1,762 patients receiving HMA, BSC, or LDAC between January 2015 and December 2018.8
Results8
Patient characteristics are summarized in Table 1.
Table 1. Patient characteristics*
|
AML, acute myeloid leukemia; BSC, best supportive care; ECOG-PS, Eastern Cooperative Oncology Group performance status; HMA, hypomethylating agents; LDAC, low-dose cytarabine. |
|
|
Characteristic |
N = 1,762 |
|---|---|
|
Therapy, % |
|
|
BSC only |
26 |
|
HMA |
62 |
|
LDAC |
15 |
|
Other systemic therapies |
23 |
|
Male, % |
57 |
|
Median age, years (range) |
75 (20–89) |
|
Secondary AML, % |
32 |
|
ECOG-PS |
|
|
0–1 |
38 |
|
≥2 |
43 |
|
Unknown |
19 |
|
Molecular mutation, % |
17 |
|
Cytogenetic risk, % |
|
|
Favorable |
12 |
|
Intermediate |
32 |
|
Poor |
25 |
|
Unknown |
30 |
Median progression-free survival (PFS) in the overall population was 4.7 months. The median time-to-treatment failure (TTF), OS, and PFS by therapy are summarized in Figure 2.
Figure 2. Median TTF, PFS, and OS*
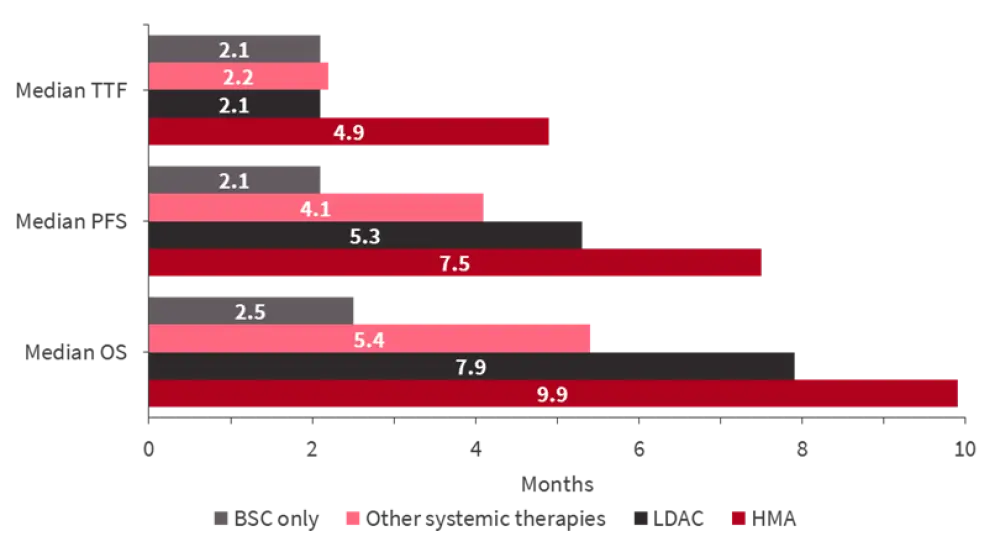
BSC, best supportive care; HMA, hypomethylating agent; LDAC, low-dose cytarabine; OS, overall survival; PFS, progression-free survival; TTF, time-to-treatment failure.
*Adapted from Kondo et al.8
The complete remission/complete remission with incomplete hematologic recovery rate was 19%, 27%, and 21% with HMA, LDAC, and other systemic therapies, respectively. The median time to best response was 115, 55, and 41 days, respectively.
In summary, real-world data gathered in that study8 was in line with clinical trials demonstrating poor OS for patients with AML who are ineligible for intensive chemotherapy. For that patient population, the development of novel agents or combination therapies remains an unmet clinical need.
Further approaches for patients ineligible for intensive chemotherapy
Venetoclax
A notable change to induction formulations for patients ineligible for intensive chemotherapy is the addition of venetoclax to azacitidine, decitabine, and LDAC. The FDA granted these combinations approval in 2020 following results of the pivotal phase III VIALE-A (NCT02993523) and VIALE-C (NCT03069352) trials, demonstrating a significant reduction in the risk of death, increased median OS and CR rate when compared to azacitidine or LDAC alone.9
Real-world comparisons of HMA + venetoclax have demonstrated comparable OS and complete remission/complete remission with incomplete hematologic recovery with liposomal formulation of daunorubicin and cytarabine (CPX-351), given to older fit patients. CPX-351 was associated with higher rate of adverse events such as febrile neutropenia, infection, and increased hospital stay.10 Despite study limitations, the survival outcomes of a more tolerable treatment for unfit patients are encouraging to help guide treatment options when it is difficult to define patient fitness. Replication of prospective trials will be needed.
What does real-world data tell us about frontline therapy with CPX-351 vs venetoclax + azacitidine?
However, improved response rates were not reached in patients with poor-risk cytogenetics who harbor TP53 mutations, with recent data presented at the 63rd ASH Annual Meeting and Exposition (ASH 2021) revealing no significant difference in the median duration of response (DoR) in patients with TP53mut treated with venetoclax + azacitidine (6.54 months) versus azacitidine alone (6.7 months).11
FLT3 inhibitors
The addition of FLT3 inhibitors to low-intensity chemotherapy is still a clinical approach in its infancy. In a phase I/II trial, including a newly diagnosed FLT3-ITD-mutated AML cohort, patients were treated with quizartinib, a FLT3 inhibitor, in combination with venetoclax and decitabine. All patients achieved a response. In a median follow-up duration of 16 months, the median OS was 14.5 months.12
Conclusion
While challenges around improved survival remain, the outlook of non-intensive induction therapy for AML has evolved in recent years with the approval of targeted agents, particularly the addition of venetoclax to HMAs and LDAC. Growing clinical data has demonstrated improved outcomes when certain targeted therapies are added to intensive chemotherapeutic backbones, thus, potentially leading to improved individualization of induction therapy strategies in the future.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?