All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View AML content recommended for you
Enasidenib or ivosidenib in combination with intensive chemotherapy in patients with newly diagnosed AML
Isocitrate dehydrogenase (IDH)1 and 2 gene mutations are frequently seen in patients with acute myeloid leukemia (AML). These IDH1 and IDH2 mutations can be targeted using ivosidenib or enasidenib, respectively, which act as small molecule inhibitors. Overall response rates of ~40% have been achieved in phase I trials of either ivosidenib or enasidenib used alone; therefore, investigators decided to assess the benefit of combining these treatments with chemotherapy.
Eytan Stein and colleagues published an article in Blood on the results of a phase I trial (NCT02632708) of enasidenib or ivosidenib combined with intensive induction and consolidation chemotherapy in patients with newly diagnosed AML.1
Study design
In this phase I trial, four treatment arms were assessed as shown in Figure 1. Initially, six patients were enrolled in each arm of the trial. If two or fewer patients experienced a dose limiting toxicity (DLT), six more patients would be enrolled on that arm. Out of this cohort of 12, if less than of equal to three patients experienced a DLT this dose was taken forward for evaluation. If these conditions were not met, a lower dose was administered.
Figure 1. Study design for the initial phase of testing*
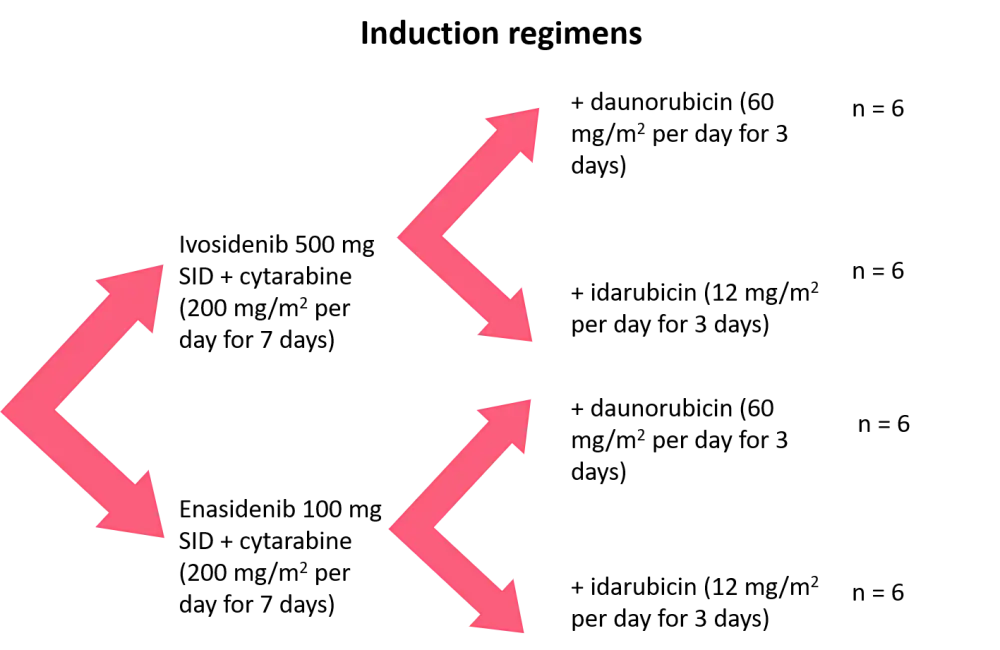
SID, once a day.
*Data from Stein et al.1
If patients achieved at least a partial response by the end of induction they were given consolidation therapy as follows:
- up to four cycles of intermediate- or high-dose cytarabine or one cycle of mitoxantrone/etoposide;
- plus ivosidenib or enasidenib continuously once daily.
Maintenance therapy was given to patients in remission at the end of consolidation, consisting of:
- ivosidenib or enasidenib continuously once daily until relapse/unacceptable toxicity or allogeneic stem cell transplant (allo-SCT).
The eligibility criteria included:
- patients aged ≥18 years diagnosed with AML (de novo or secondary);
- Eastern Cooperative Oncology Group score of 0–2; and
- IDH1 or IDH2 mutation by laboratory testing.
Patients were ineligible if:
- they had received prior chemotherapy for AML (except hydroxyurea).
The primary endpoint of this trial was the safety and tolerability of the combinations tested.
Results
In the ivosidenib + chemotherapy arm:
- 15% received two cycles of induction;
- 58% went on to consolidation therapy; and
- 32% received ivosidenib maintenance.
With respect to treatment continuation, 78% of the ivosidenib cohort discontinued (mostly to receive allo-SCT; 28 patients).
In the enasidenib + chemotherapy arm:
- 24% received two cycles of induction;
- 49% went on to consolidation therapy; and
- 26% received enasidenib maintenance.
Regarding treatment continuation, 87% of the enasidenib cohort discontinued (mostly to receive allo-SCT; 43 patients).
Patient baseline characteristics are shown in Table 1. The median age was around 63 years in both cohorts and the majority of patients were diagnosed with de novo AML. In the enasidenib arm, almost 50% of patients (with secondary AML) had received a hypomethylating agent, compared with only 22% in the ivosidenib arm.
Table 1. Baseline patient characteristics*
|
AML, acute myeloid leukemia; IDH, isocitrate dehydrogenase. |
||
|
Characteristic |
Ivosidenib 500 mg + chemotherapy |
Enasidenib 100 mg + chemotherapy |
|---|---|---|
|
Median age, years (range) |
62.5 (24–76) |
63.0 (27–77) |
|
Age category, % |
|
|
|
Male, % |
50 |
56 |
|
Type of AML, % |
|
|
|
Prior hypomethylating agent, %† |
22 |
49 |
|
IDH1 mutation type, %‡ |
|
|
|
IDH2 mutation type, %‡ |
|
|
|
Cytogenetic risk status by investigator, % |
|
|
Efficacy
Complete response (CR)/CR with incomplete neutrophil recovery (CRi)/CR with incomplete platelet (CRp) rates were similar between treatment arms (ivosidenib, 77%; enasidenib, 74%), with patients with de novo AML achieving higher rates than patients diagnosed with secondary AML (Table 2). In the ivosidenib cohort, 68% of patients achieved CR, compared with 55% in the enasidenib arm.
Table 2. Overall responses*
|
AML, acute myeloid leukemia; CR, complete response; CRi, complete response with incomplete neutrophil recovery; CRp, complete response with incomplete platelet recovery; MLFS, morphologic leukemia-free state; PR, partial response. |
||||||
|
Response category, % |
Ivosidenib 500 mg + chemotherapy |
Enasidenib 100 mg + chemotherapy |
||||
|---|---|---|---|---|---|---|
|
All |
De novo AML |
Secondary AML |
All |
De novo AML |
Secondary AML |
|
|
CR/CRi/CRp |
77 |
88 |
50 |
74 |
80 |
63 |
|
CR |
68 |
76 |
50 |
55 |
64 |
40 |
|
CRi/CRp |
8 |
12 |
— |
19 |
16 |
23 |
|
MLFS |
7 |
7 |
6 |
11 |
9 |
14 |
|
PR |
3 |
— |
11 |
2 |
2 |
3 |
|
Treatment failure |
13 |
5 |
33 |
13 |
9 |
20 |
Median overall survival was not reached for the ivosidenib arm after a median follow-up of 9.3 months (range, 0.4–32.1 months).
In the enasidenib arm, median overall survival was 25.6 months (95% confidence interval, 25.5 months–not calculable) after a median follow-up of 14.5 months (range, 0.5−31.8 months).
IDH-1/2-clearance was assessed in the patients with best response of CR/CRi/CRp. For the ivosidenib group, 39% had IDH1 mutant clearance from the bone marrow, as assessed by polymerase chain reaction. In the enasidenib group, 23% had IDH2 mutant clearance.
Measurable residual disease (MRD) was assessed by multiparameter flow cytometry in patients with best response of CR/CRi/CRp:
- 80% of the ivosidenib arm were MRD negative; and
- 63% of the enasidenib arm were MRD negative.
The most frequent baseline mutations were:
- DNMT3A (41%), NPM1 (34%), ASXL1 (20%), and BCOR (14%) in the ivosidenib arm; and
- DNMT3A (39%), SRSF2 (25%), ASXL1 (23%), and RUNX1 (20%) in the enasidenib arm.
ASXL1, NRAS, U2AF1, and TP53 were associated with a lack of CR/CRi/CRp only in the enasidenib arm.
Safety
Only one DLT was recorded during the initial safety evaluation. A 64-year-old man with de novo AML developed persistent Grade 4 thrombocytopenia on Day 42 of Cycle 1.
Both treatment arms exhibited a similar median time to recovery of absolute neutrophil count and platelet count of 28 days.
The most common non-hematologic treatment emergent adverse events (TEAEs) were diarrhea, nausea, and rashes (Table 3). The majority of TEAEs were Grade <3. The most frequent Grade ≥3 TEAEs were increased blood bilirubin (16.1% in the enasidenib arm) and hypophosphatemia (16.7% in the ivosidenib arm).
In the ivosidenib arm, the 30-day mortality rate was 5%, increasing to 10% at 60-days. Results were similar in the enasidenib arm, at 5% and 9% for the 30- and 60-day mortality rates, respectively.
During this trial, 13 patients in the ivosidenib arm died and 31 deaths occurred in the enasidenib cohort. None of the deaths were considered to be related to treatment.
Table 3. Non-hematologic TEAEs experienced in >30% of patients in any treatment arm*
|
TEAE, treatment-associated adverse event. |
||||||||
|
TEAE, % |
Induction period |
Consolidation period |
||||||
|---|---|---|---|---|---|---|---|---|
|
Ivosidenib 500 mg + chemotherapy |
Enasidenib 100 mg + chemotherapy |
Ivosidenib 500 mg + chemotherapy |
Enasidenib 100 mg + chemotherapy |
|||||
|
All |
Grade ≥3 |
All |
Grade ≥3 |
All |
Grades ≥ 3 |
All |
Grade ≥3 |
|
|
Any |
100.0 |
96.7 |
98.9 |
93.5 |
100.0 |
97.1 |
97.8 |
89.1 |
|
Diarrhea |
71.7 |
1.7 |
59.1 |
5.4 |
20.0 |
0.0 |
37.0 |
0.0 |
|
Nausea |
55.0 |
0.0 |
53.8 |
2.2 |
31.4 |
0.0 |
32.6 |
2.2 |
|
Rash† |
55.0 |
5.0 |
54.8 |
14.0 |
34.3 |
2.9 |
28.3 |
2.2 |
|
Reduced appetite |
53.3 |
8.3 |
33.3 |
3.2 |
11.4 |
0.0 |
23.9 |
2.2 |
|
Vomiting |
35.0 |
0.0 |
33.3 |
1.1 |
25.7 |
2.9 |
21.7 |
0.0 |
|
Stomatitis |
33.3 |
5.0 |
24.7 |
4.3 |
11.4 |
0.0 |
19.6 |
8.7 |
|
Fatigue |
31.7 |
0.0 |
25.8 |
2.2 |
14.3 |
0.0 |
19.6 |
4.3 |
|
Hypokalemia |
28.3 |
11.7 |
31.2 |
9.7 |
8.6 |
2.9 |
23.9 |
8.7 |
|
Pyrexia |
26.7 |
6.7 |
33.3 |
2.2 |
22.9 |
2.9 |
28.3 |
0.0 |
|
Peripheral edema |
23.3 |
0.0 |
39.8 |
0.0 |
5.7 |
0.0 |
28.3 |
0.0 |
|
Headache |
16.7 |
0.0 |
31.2 |
0.0 |
17.1 |
2.9 |
17.4 |
0.0 |
|
Blood bilirubin increased‡ |
18.3 |
6.7 |
49.5 |
16.1 |
5.7 |
2.9 |
28.3 |
10.9 |
In the ivosidenib arm, two patients developed IDH-differentiation syndrome (DS). The same was true in the enasidenib arm, and all four cases occurred during induction. IDH-DS was resolved in three of the patients and they went on to achieve CR. The remaining patient died as a result of a lung infection and had ongoing IDH-DS at the time of death.
QT prolongation in the ivosidenib cohort was reported in 26.7% and 10% experienced Grade ≥3 QT prolongation. In the enasidenib group, three patients reported QT prolongation and in one case it was Grade ≥3.
Mitoxantrone/etoposide was only used in two patients, therefore the safety of this consolidation treatment could not be assessed.
Conclusion
This phase I study demonstrated that the IDH inhibitors in combination with intensive induction and consolidation chemotherapy were well tolerated in both arms. CR/CRi/CRp rates were >70% in both the ivosidenib and enasidenib arms. A further phase III trial is being conducted to assess the value of ivosidenib or enasidenib and chemotherapy for newly diagnosed patients with IDH-mutant AML.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?