All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Kura Oncology, Syndax, Abbvie, Thermo Fisher and Johnson & Johnson. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Symposium | Comparing treatment options for patients with FLT3-ITD and -TKD mutations
Featured:
 Jorge Cortes
Jorge CortesDo you know... How do Type I and Type II FLT3 inhibitors differ in their activity against FLT3-ITD and FLT3-TKD mutations?
The AML Hub held a virtual symposium on November 19, 2025, titled Understanding the differences between FLT3-ITD and -TKD mutations in AML: Implications for clinical practice. Here, we share a presentation from the symposium by Jorge Cortes, Georgia Cancer Center, Augusta, US, comparing treatment options for patients with FLT3-ITD and -TKD mutated acute myeloid leukemia (AML).
Symposium | Comparing treatment options for patients with FLT3-ITD and -TKD mutations
Symposium | Comparing treatment options for patients with FLT3-ITD and -TKD mutations
Cortes described the mechanisms of action of Type I and Type II FLT3 inhibitors, before going on to discuss key efficacy and survival data from clinical trials of FLT3-targeted therapies, both as monotherapies and in combination strategies for the treatment of FLT3-ITD and FLT3-TKD-mutated AML. Cortes concluded with an overview of novel therapeutic strategies in AML treatment.
Key points
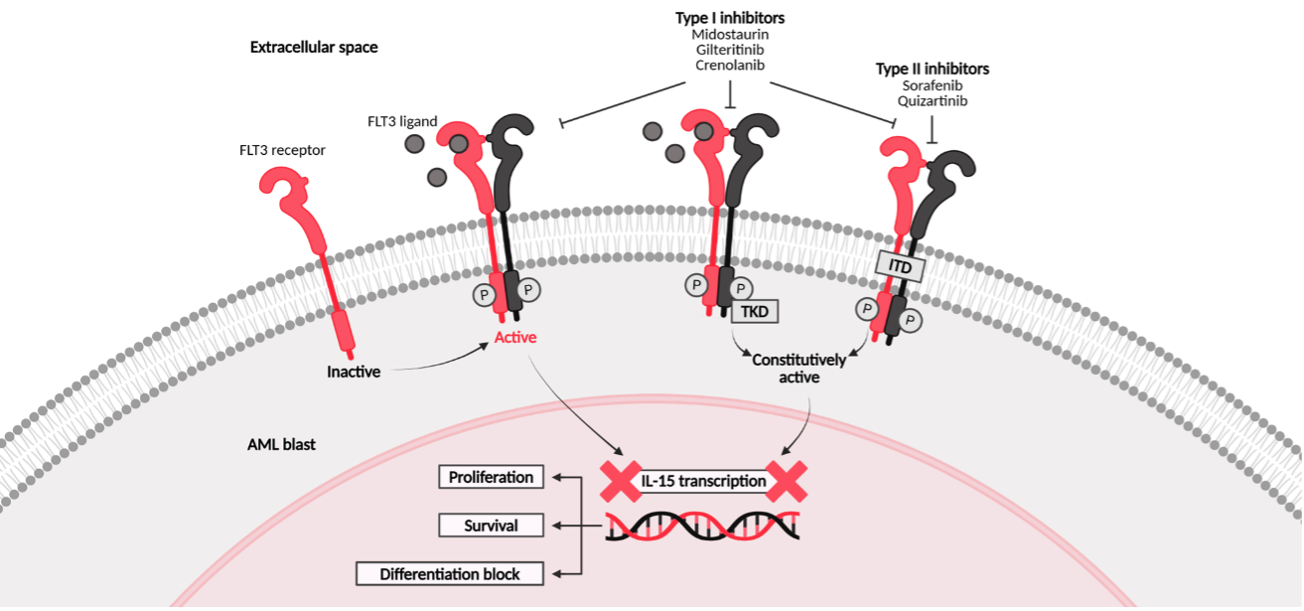
- FLT3 inhibitors are classified as Type I or Type II (Figure 1).1
- Type I FLT3 inhibitors, such as midostaurin, gilteritinib, and crenolanib, target both FLT3-ITD and FLT3-TKD.1
- Type II inhibitors, such as sorafenib and quizartinib, target FLT3-ITD only.1
Figure 1. Mechanism of action of Type I and Type II FLT3 inhibitors1
- Quizartinib and gilteritinib monotherapies have benefits over standard chemotherapy in relapsed/refractory (R/R) AML.2–4
- In the QuANTUM-R trial of quizartinib monotherapy (n = 245) vs salvage chemotherapy (n = 122) in patients with R/R FLT3-ITD AML, a higher proportion of patients achieved composite complete remission (CRc) compared with salvage (48% [95% CI, 42–55] vs 27% [95% CI, 19–36]).2
- Furthermore, median overall survival (mOS) was longer with quizartinib treatment vs salvage chemotherapy (6.2 months [95% CI, 5.3–7.2] vs 4.7 months [95% CI, 4.0–5.5]; p = 0.02), as was median event-free survival (mEFS; 1.4 months [95% CI, 0.0–1.9] vs 0.0 [95% CI, 0.0–1.0]; p = 0.01).2
- In the ADMIRAL trial of gilteritinib (n = 247) vs salvage chemotherapy (n = 124) in patients with R/R FLT3-ITD or -TKD AML, CRc rates were higher (54% vs 22%), and mOS significantly prolonged (9.3 months [95% CI, 7.7–10.7] vs 5.6 months [95% CI, 4.7–7.3]; p = 0.001).3
- Gilteritinib has also shown potent antiproliferative activity against FLT3-TKD mutations, including those associated with resistance to Type II FLT3 inhibitors.4
- Both midostaurin and quizartinib, in combination frontline strategies in patients with FLT3-mutated AML, improve survival compared with chemotherapy alone.
- In the RATIFY trial of midostaurin (n = 360) vs placebo (n = 357) with standard chemotherapy in patients with newly diagnosed (ND) FLT3-ITD or -TKD AML, mEFS was prolonged with midostaurin vs placebo (8.2 months vs 3.0 months; HR, 0.78 [95% CI, 0.66–0.93]).5
- The 10-year follow-up analysis of the RATIFY trial demonstrated a durable survival benefit with midostaurin vs placebo (OS HR, 0.82 [95% CI, 0.67–1.00]; EFS HR, 0.79 [95% CI, 0.67–0.94]).6
- In the QuANTUM-First trial of quizartinib (n = 268) vs placebo (n = 271) with standard chemotherapy in patients with ND FLT3-ITD AML, the primary endpoint was met, with clinically meaningful improvements in OS demonstrated (mOS, 31.9 months [95% CI, 21.0–NE] vs 15.1 months [95% CI, 13.2–26.2]; HR, 0.78 [95% CI, 0.62–0.98]; p = 0.032).7
- In the LACEWING trial in patients with ND FLT3-mutated AML, gilteritinib in combination with azacitidine (n = 74) did not demonstrate a survival benefit vs azacitidine alone (n = 49). At a median follow-up of 9.76 months vs 17.97 months respectively, mOS was 9.82 months (95% CI, 7.56–12.55) vs 8.87 months (95% CI, 4.34–14.03; HR, 0.916 [95% CI, 0.529–1.585]; p = 0.753).8
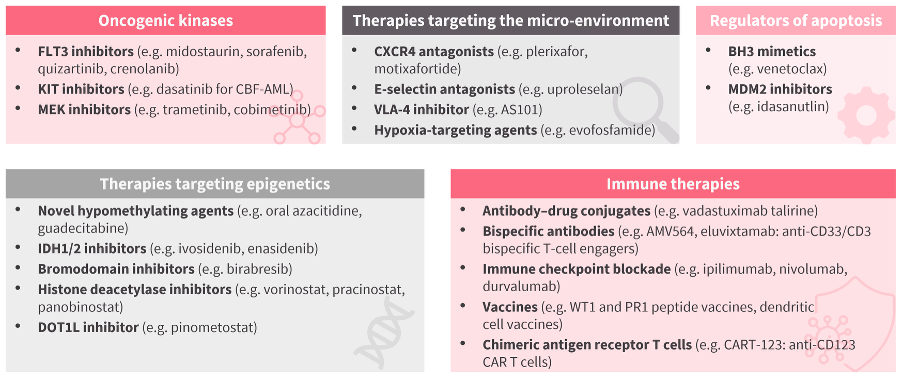
- In addition to FLT3 inhibitors, investigation into further novel therapeutic strategies for AML treatment is ongoing (Figure 2).
Figure 2. Novel therapeutic strategies in AML treatment9
This educational resource is independently supported by Daiichi Sankyo. All content was developed by SES in collaboration with an expert steering committee. Funders were allowed no influence on the content of this resource.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
More from this series:
Symposium series | Understanding the differences between FLT3-ITD and -TKD mutations in AML: Implications for clinical practice




Your opinion matters
What is the typical turnaround time for next-generation sequencing (NGS) results for AML at your center?