All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Kura Oncology, Syndax, Abbvie, Thermo Fisher and Johnson & Johnson. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Treatment decisions in AML: Personalizing care with FLT3 inhibitor therapy
Featured:
 Jeffrey Lancet
Jeffrey Lancet Uwe Platzbecker
Uwe Platzbecker Agnieszka Wierzbowska
Agnieszka Wierzbowska Charles Craddock
Charles Craddock Roland Walter
Roland Walter Hee-Je Kim
Hee-Je Kim Jorge Sierra
Jorge Sierra Yasushi Miyazaki
Yasushi Miyazaki Jorge Cortes
Jorge CortesDo you know... Which of the following statements correctly describes the ELN risk classification for patients with FLT3-ITD AML?
During a meeting of the AML Hub Steering Committee, held on February 19, 2026, Jorge Sierra chaired a discussion on the topic, Treatment decisions in AML: Personalizing care with FLT3 inhibitor therapy. The discussion featured contributions from Charles Craddock, Jorge Cortes, Hee-Je Kim, Jeffrey Lancet, Yasushi Miyazaki, Uwe Platzbecker, Roland Walter, and Agnieszka Wierzbowska.
Treatment decisions in AML: Personalizing care with FLT3 inhibitor therapy
Treatment decisions in AML: Personalizing care with FLT3 inhibitor therapy
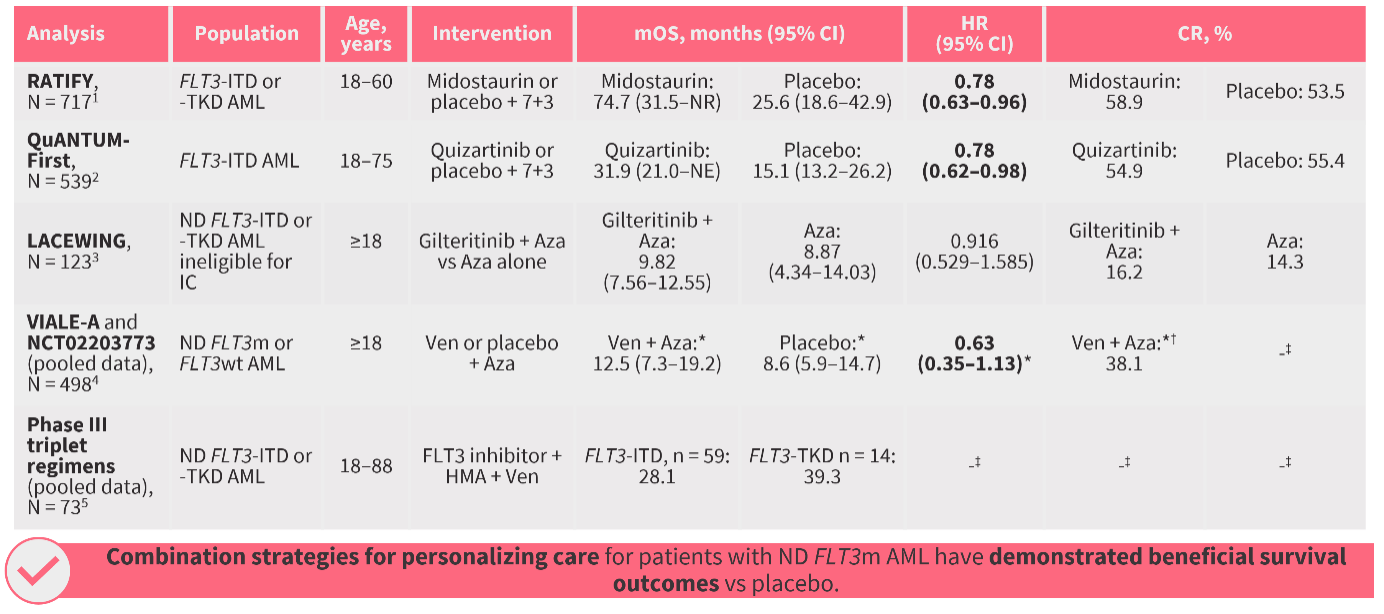
Sierra first provided an overview of the role of FLT3 mutations in acute myeloid leukemia (AML) pathogenesis, and highlighted key considerations when making treatment decisions for patients with FLT3-mutated (FLT3m) AML, such as the European Leukemia Network (ELN) 2022 and 2024 risk classifications (Figure 1). He summarized key combination strategies for the treatment of AML (Figure 2), and shared updates from the 67th American Society of Hematology Annual Meeting and Exposition and the European Hematology Association 2025 Congress on triplet regimens including the FLT3 inhibitors gilteritinib and quizartinib. The discussion centered around preferred approaches to personalizing care in two patient cases.
Figure 1. Risk classifications for patients with FLT3m AML
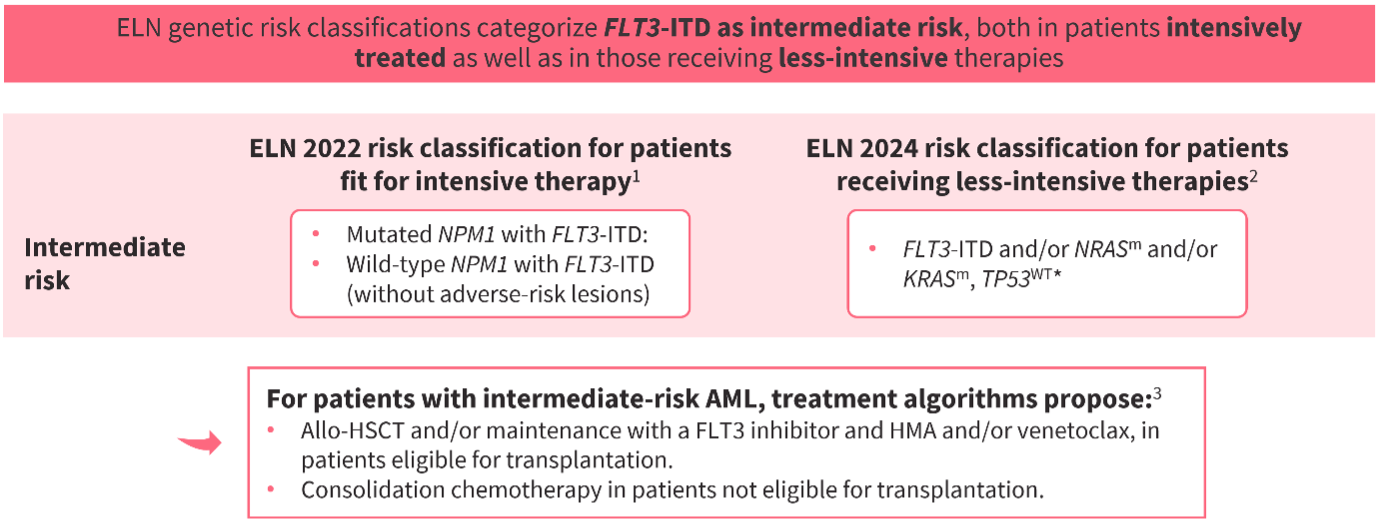
Figure 2. Data supporting combination strategies for the treatment of FLT3m AML
Key points
First-line treatment strategy in a 60-year-old fit patient with FLT3-ITD AML, with concomitant NPM1 and DNMT3A mutations
- The preferred treatment approach would be 7+3 plus a FLT3 inhibitor; promising safety and efficacy data have been reported with quizartinib in this population, in the QuANTUM-First trial (NCT02668653).5
- If measurable residual disease (MRD)-positive complete remission (CR) or CR with incomplete hematologic recovery (CRi) following induction and consolidation was achieved, proceeding directly to allogeneic hematopoietic stem cell transplantation (allo-HSCT) with FLT3 inhibitor maintenance would be preferred, given uncertainty around whether attempts to convert MRD positivity to negativity prior to transplantation would translate into meaningful survival benefits.
- Optimal selection of post-transplantation maintenance therapy remains an unmet clinical need. Gilteritinib is well supported by evidence; however, studies investigating quizartinib for post-transplantation maintenance in FLT3-ITD AML are underway.
- In MRD-negative CR/CRi after induction and consolidation, an MRD-guided approach, with transplantation delayed until MRD positivity recurred, or consideration of allo-HSCT if the patient was fit and had a suitable donor, was discussed.
First-line treatment strategy in a 70-year-old unfit patient with FLT3-ITD AML, with concomitant SF3B1 and IDH1 mutations
- The preferred approach would be a triplet combination of venetoclax (Ven) + azacitidine (Aza) and a FLT3 inhibitor.
- Greater long-term benefit has been demonstrated with such triplet regimens than with Ven + Aza doublet regimens in patients with FLT3-ITD AML.9
- Important considerations for managing FLT3m AML with triplet regimens include close monitoring for myelosuppression and toxicity.
- If MRD-positive CR was achieved, initial therapy should be continued, due to the variability in fitness and treatment tolerance, and potential for rapid clinical deterioration, in older patient populations.
This educational activity is independently supported by Daiichi Sankyo. All content was developed by the faculty in collaboration with SES. Funders were allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the typical turnaround time for next-generation sequencing (NGS) results for AML at your center?

.jpeg&w=3840&q=75)
