All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Kura Oncology, Syndax, Abbvie, Thermo Fisher and Johnson & Johnson. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Optimizing induction regimens in younger patients with AML: The UK AML19 trial
The phase III UK National Cancer Research Institute AML19 trial (ISRCTN78449203) aimed to determine the optimal induction chemotherapy regimen in younger patients with newly diagnosed acute myeloid leukemia (AML) without adverse risk cytogenetics.1 Here, we summarize results from this trial, published by Russell et al.1 in the Journal of Clinical Oncology.
Study design and patient population1
- In total, 1,479 patients with newly diagnosed AML or myelodysplastic syndrome with excess blasts 2 were randomized to receive either fludarabine, cytarabine, granulocyte colony-stimulating factor, and idarubicin (FLAG-Ida; n = 738) or daunorubicin and cytarabine (DA, n = 741).
- Of these, 1,033 were randomized to receive single dose gemtuzumab ozogamicin (GO) on Day 1 (GO1, n = 514) or a fractionated dosing schedule on Day 1 and Day 4 (GO2, n = 519).
- Median age was 51.5 years, with 14% of patients aged >60 years.
- Overall, 30%, 26%, and 12% of patients had NMP1-mutated, FLT3-mutated, or core binding factor-AML, respectively.
- The primary endpoint was overall survival (OS)
Key findings1
- There was no difference between response rates and survival outcomes in patients randomized to GO1 or GO2; therefore, these groups were combined for comparisons between FLAG-Ida + GO and DA + GO.
Induction response
- Both response rates after two courses, and 30- and 60-day early mortality rates, were similar between treatment arms (Table 1).
- More patients treated with DA + GO underwent allogeneic hematopoietic stem cell transplantation vs FLAG-Ida + GO (Table 1).
Table 1. Response, early mortality, and allo-HSCT rates between DA + GO vs FLAG-Ida + GO in the AML19 trial*
|
Outcome, % |
DA + GO |
FLAG-Ida + GO |
p-value |
|---|---|---|---|
|
Response after Cycle 1 |
|||
|
CR |
66 |
76 |
0.014 |
|
CRi |
11 |
9 |
|
|
ORR |
78 |
85 |
|
|
Best response after two cycles |
|||
|
CR |
87 |
87 |
0.19 |
|
CRi |
3.9 |
5.7 |
|
|
ORR |
91 |
93 |
|
|
Early mortality |
|||
|
Day 30 |
2.9 |
3.1 |
0.83 |
|
Day 60 |
4.6 |
4.3 |
0.80 |
|
Allo-HSCT |
|||
|
Allo-HSCT at any time |
54 |
46 |
0.021 |
|
Allo-HSCT in first response† |
42 |
38 |
0.22 |
|
Allo-HSCT, allogeneic hematopoietic stem cell transplantation; CR, complete remission; CRi, CR with incomplete count recovery; DA, daunorubicin and cytarabine; FLAG-Ida, fludarabine, cytarabine, granulocyte colony-stimulating factor, and idarubicin; GO, gemtuzumab ozogamicin; ORR, overall response rate. *Adapted from Russell, et al.1 †Percentage of patients achieving CR/CRi. |
|||
Survival outcomes
- When compared with DA + GO, FLAG-Ida + GO reduced relapse, improved event-free survival (EFS), and relapse-free survival (Figure 1).
- OS was similar between treatment arms, and the cumulative incidence of death in remission was higher with FLAG-Ida + GO vs DA + GO (Figure 1).
Molecular subgroup analysis
- Treatment with FLAG-Ida + GO improved OS vs DA + GO in patients with NPM1 mutations, and in those with FLT3 mutations, but not in patients with core binding factor-AML (Figure 1).
- FLAG-Ida + GO was also associated with achievement of measurable residual disease negativity after course two vs DA + GO in the peripheral blood (88% vs 77%; p = 0.02) and the bone marrow (56% vs 37%; p = 0.004).
Figure 1. 3-year survival outcome rates by treatment arm in the AML19 trial in A all patients and B within molecular subgroups*
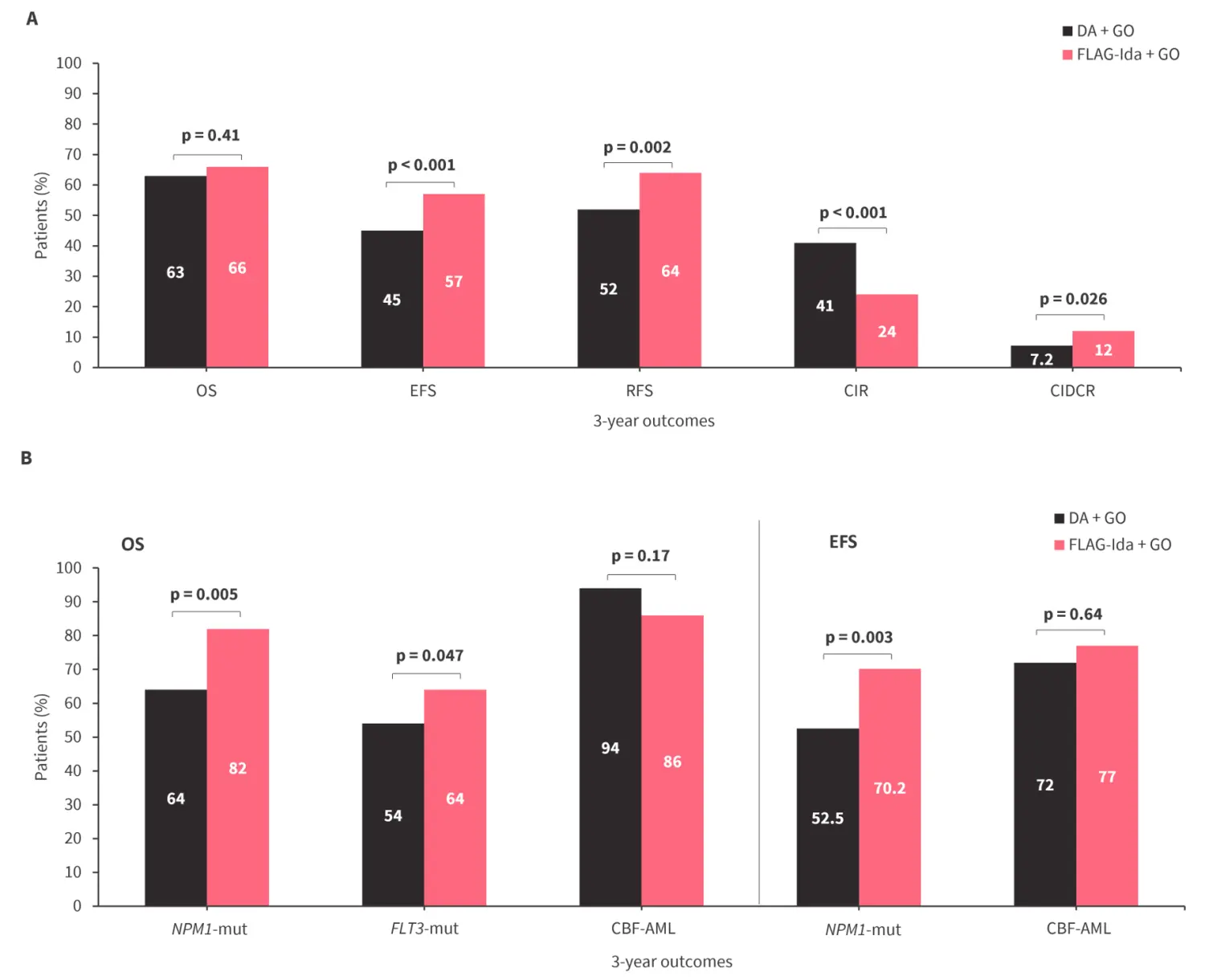
AML, acute myeloid leukemia; CBF-AML, core binding factor-AML; CIDCR, cumulative incidence of death in remission; CIR, cumulative incidence of relapse; DA, daunorubicin and cytarabine; EFS, event-free survival; FLAG-Ida, fludarabine, cytarabine, granulocyte colony-stimulating factor, and idarubicin; GO, gemtuzumab ozogamicin; mut, mutated; OS, overall survival; RFS, relapse-free survival.
*Data from Russell, et al.1
Safety
- After course two, FLAG-Ida + GO was associated with a longer median time to neutrophil recovery (40 vs 27 days; p <0.001) and time to platelet recovery (46 vs 28 days; p <0.001) vs DA + GO.
- When comparing GO1 and GO2, time to neutrophil recovery (median, 29 vs 29 days; p = 0.23) and to platelet recovery (median, 27 vs 29 days; p = 0.07) were similar.
|
Key learnings |
|
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the typical turnaround time for next-generation sequencing (NGS) results for AML at your center?


