All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Reduced-intensity transplantation in older patients with acute myeloblastic leukemia: NCRI AML16 trial
Treatment of older patients with acute myeloid leukemia (AML) remains a challenge as these patients are more vulnerable and often have more aggressive malignancies than younger patients. The incidence of AML increases with age, with more than half of patients diagnosed when aged >65 years. Current treatments for older patients have not shown the improvements in survival that have been achieved in younger patients. A benefit of reduced-intensity conditioning (RIC) transplantation over chemotherapy has been reported in patients aged 40–59 years. Thus, with the superior potential of RIC regimens, this therapy has been increasingly applied to older patients with AML.
The National Cancer Research Institute (NCRI) AML16 trial (NCT00454480; EUDRACT 2005-002847-14) is a randomized, multi-arms phase II/III trial comparing different combination chemotherapy regimens and RIC transplantation in older patients (>60 years) with AML and high-risk myelodysplastic syndromes (MDS). Early outcomes showed that induction chemotherapy with gemtuzumab ozogamicin (GO) reduced relapse risk and improved survival in older patients. The latest results, comparing RIC transplantation with chemotherapy in older patients, were recently published in Haematologica by Russell, et al.1 Below, we summarize the key findings.
Methods and patients
A total of 932 patients who were in remission after Course 1 and without favorable-risk cytogenetics were eligible to undergo RIC transplantation from either a matched sibling or matched unrelated donor (MUD). Of the 144 RIC transplants performed, 52 were from matched sibling donors and 92 were from a MUD. The other 788 patients received chemotherapy alone. Overall, 83% of patients had intermediate-risk cytogenetics and 17% of patients had adverse-risk cytogenetics. The median time from complete remission to transplant was 110 days. The median follow-up for survival from remission was 60 months.
The study design and patient characteristics are detailed in Figure 1 and Table 1, respectively.
Figure 1. Study design*
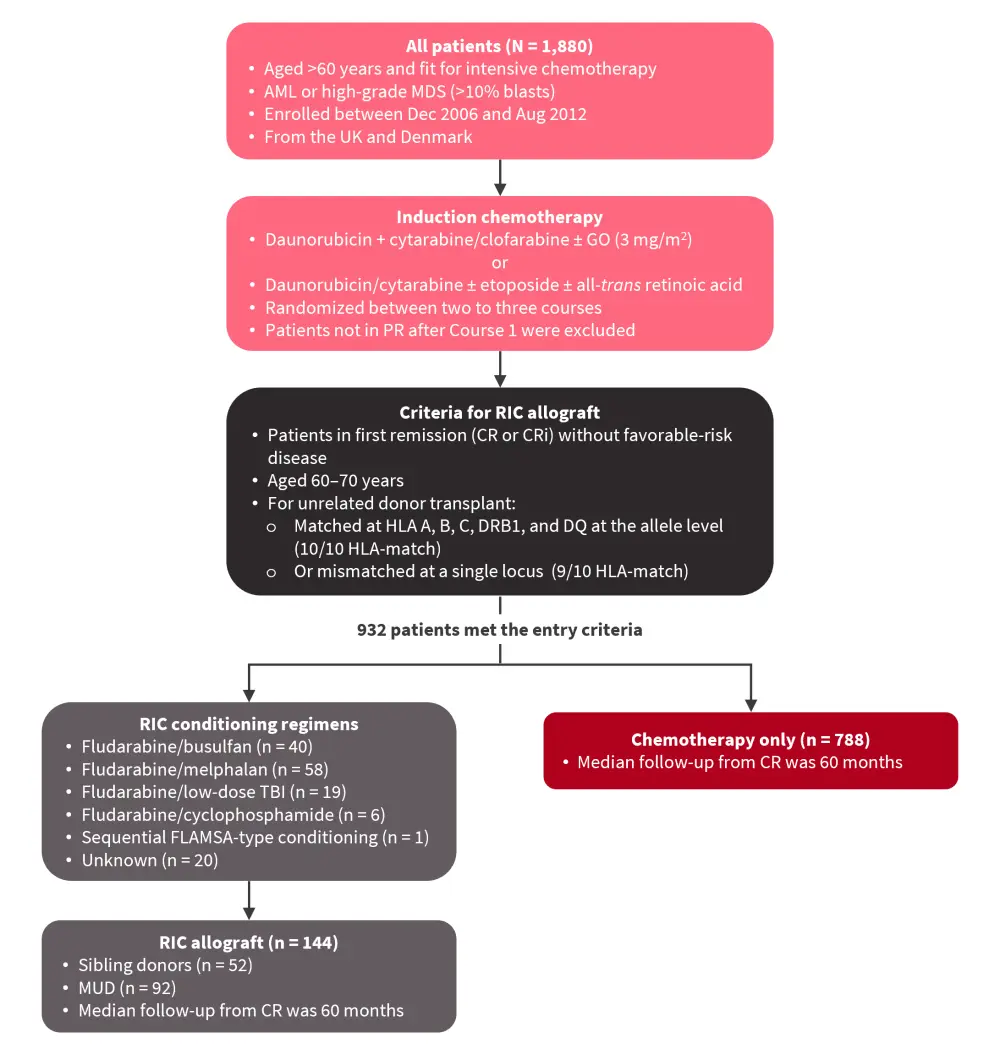
AML, acute myeloid leukemia; CR, complete remission; CRi, incomplete CR; FLAMSA, fludarabine, amsacrine, and cytarabine; GO, gemtuzumab ozogamicin; HLA, human leukocyte antigen; MDS, myelodysplastic syndromes; MUD, matched unrelated donor; PR, partial remission; RIC, reduced-intensity conditioning; TBI, total body irradiation.
*Adapted from Russell, et al.1
Table 1. Baseline characteristics*
|
HCT-CI, Hematopoietic Cell Transplantation Comorbidity Index; ITD, internal tandem duplication; MDS, myelodysplastic syndromes; Q1, first quartile; Q3, third quartile; WHO, World Health Organization; WT, wild type. |
||||
|
Characteristic, % (unless otherwise stated) |
Overall |
No allograft |
Allograft |
p value† |
|---|---|---|---|---|
|
Median age, years (Q1–Q3) |
65 (63–68) |
66 (63–68) |
64 (62–66) |
|
|
60–65 years |
51 |
48 |
69 |
<0.001 |
|
66–70 years |
49 |
52 |
31 |
<0.001‡ |
|
Sex |
|
|
|
|
|
Male |
58 |
57 |
65 |
0.062 |
|
Female |
42 |
43 |
35 |
|
|
WHO performance status |
|
|
|
|
|
0 |
62 |
60 |
76 |
<0.001§ |
|
1 |
33 |
35 |
23 |
|
|
2 |
3 |
3 |
1 |
|
|
3 |
2 |
2 |
1 |
|
|
Diagnosis |
|
|
|
|
|
De novo |
74 |
76 |
65 |
0.012 |
|
Secondary |
14 |
14 |
17 |
|
|
High-risk MDS |
12 |
10 |
18 |
|
|
Cytogenetics |
|
|
|
|
|
Intermediate |
83 |
83 |
84 |
0.868 |
|
Adverse |
17 |
17 |
16 |
|
|
Unknown, n |
204 |
171 |
33 |
|
|
Risk group |
|
|
|
|
|
Good |
49 |
48 |
58 |
0.013§ |
|
Standard |
29 |
29 |
27 |
|
|
Poor |
22 |
23 |
15 |
|
|
HCT-CI score |
|
|
|
|
|
0 |
51 |
50 |
50 |
0.016§ |
|
1 or 2 |
34 |
34 |
34 |
|
|
≥3 |
15 |
16 |
9 |
|
|
FLT3-ITD |
|
|
|
|
|
WT |
82 |
81 |
90 |
0.105 |
|
Mutant |
18 |
19 |
10 |
|
|
Fail, n |
9 |
6 |
3 |
|
|
Unknown, n |
506 |
422 |
84 |
|
|
NPM1 |
|
|
|
|
|
WT |
73 |
72 |
83 |
0.087 |
|
Mutant |
27 |
28 |
17 |
|
|
Fail, n |
14 |
11 |
3 |
|
|
Unknown, n |
535 |
447 |
88 |
|
|
Donor type |
|
|
|
|
|
Sibling |
— |
— |
36 |
— |
|
MUD |
— |
— |
64 |
|
Results
Outcomes after RIC transplants
- In the 144 transplant recipients, the 5-year overall survival (OS) after remission was 37%; this did not differ significantly between those with sibling (44%) or unrelated (34%) donors (p = 0.200) (Table 2).
- The 5-year non-relapse mortality did not differ significantly between siblings (28%) and MUD (36%) transplant recipients (p = 0.318).
- When stratified by Wheatley risk group, there was no significant difference in OS between sibling and MUD transplants in terms of good (51% vs 42%), standard (49% vs 31%), or poor (0% vs 13%) risk groups (p = 0.7).
- Of note, the incidence of severe, absent, mild, and moderate chronic graft-versus-host disease at 12 months was only 12%, 38%, 26%, and 24%, respectively.
Table 2. Survival estimates*
|
CI, cumulative incidence; CR1, first complete remission; MUD, matched unrelated donor; OS, overall survival. |
||||
|
Outcome, % |
Transplant |
No transplant† |
||
|---|---|---|---|---|
|
All transplanted patients |
Sibling donor |
MUD |
||
|
OS after CR1 |
37 |
44 |
34 |
20 |
|
Relapse-free survival |
32 |
42 |
31 |
13 |
|
CI of death in Remission 1‡ |
34 |
28 |
36 |
10 |
|
CI of relapse§ |
34 |
30 |
33 |
77 |
|
Survival by Wheatley risk group |
||||
|
Good |
45 |
51 |
42 |
26 |
|
Standard |
36 |
49 |
31 |
21 |
|
Poor |
12 |
0 |
13 |
7 |
Comparison of RIC transplantation with chemotherapy
- The OS was significantly greater with the RIC transplantation compared with the chemotherapy-only group (37% vs 20%; hazard ratio [HR], 0.67; p < 0.001) (Table 2).
- Relapse-free survival was significantly improved by transplantation (32% vs 13%; HR, 0.56; p < 0.001).
- The 5-year cumulative incidence of death in remission was 34% in the RIC group versus 10% in the chemotherapy-only group (HR, 5.02; p < 0.001, with relapse analyzed as a competing risk).
- The 5-year relapse risk was greatly reduced by transplantation (34%) versus chemotherapy alone (77%) (HR, 0.30; p < 0.001, with death analyzed as a competing risk).
- When stratified by Wheatley risk groups, there was consistent benefit for RIC transplantation across good (45% vs 26%), standard (36% vs 21%), and poor (12% vs 7%) risk groups.
- Furthermore, a survival benefit associated with RIC was observed in patients with FLT3 internal tandem duplication, or NPM1 mutations.
- In addition, when stratified by post-course 1 flow minimal residual disease (MRD) status, including MRD-negative, MRD-positive, MRD unknown, and no complete remission (CR)/incomplete CR (CRi) post-course 1, benefits were again observed for patients who underwent transplantation (HR, 0.68; p < 0.001).
Conclusion
Here, we summarized the most recent data from the NCRI AML16 trial. Russell, et al. conducted an in-depth comparison between RIC transplantation and chemotherapy in older patients with AML (aged 60–70 years) in remission and without favorable disease. The results showed overall improvements in all transplant patients compared with chemotherapy alone, including improved 5-year OS, reduced 5-year relapse risk, and consistent benefits across risk groups with RIC, suggesting that RIC transplantation is a promising option for older patients with AML lacking favorable-risk cytogenetics. Furthermore, Russell, et al. concluded that their findings point to the need for more precise risk stratification, such as detailed genomic analysis, to select older patients, particularly in intermediate-risk patients with gene mutations typical of secondary AML, for transplantation.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?