All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
CPX-351 in patients with a high risk of mortality
The treatment of patients with acute myeloid leukemia (AML) who are older or have significant co-morbidities remains challenging and carries a high risk of mortality. Older patients (> 60 years) often have secondary AML (s-AML) or therapy-related AML (t-AML), which are inherently resistant to standard chemotherapy. CPX-351 is a liposomal formulation of cytarabine and daunorubicin in a fixed 5:1 molar ratio, which has been approved by the U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA) for the treatment of adults with newly diagnosed t-AML or AML with myelodysplastic syndrome-related changes (AML-MRC).
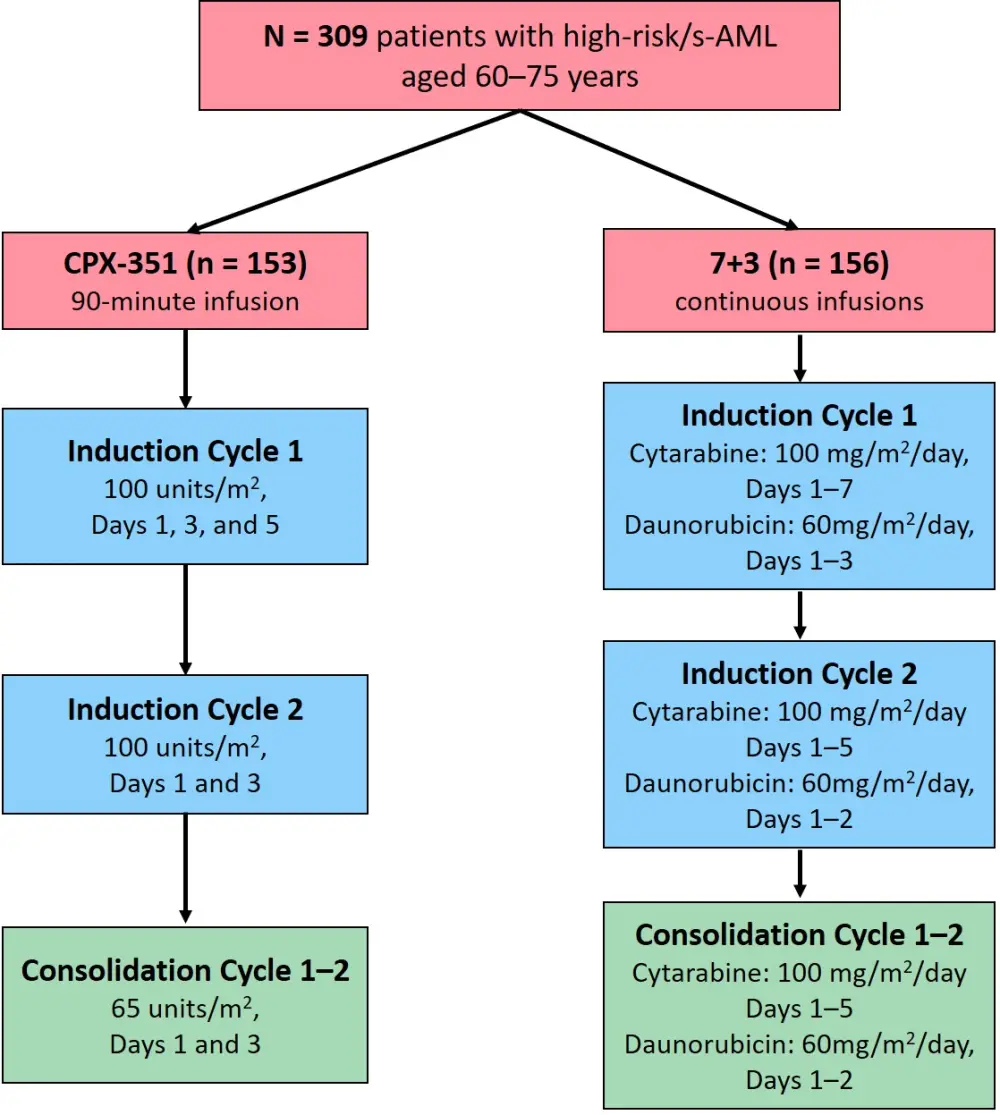
The AML Hub has previously reported on the results of the phase III trial (NCT01696084) comparing CPX-351 to standard cytarabine + daunorubicin (7+3) chemotherapy in patients with previously untreated high-risk AML/s-AML aged 60–75 years. The final 5-year results of this trial were presented at the 62nd American Society of Hematology (ASH) Annual Meeting and Exposition by Jeffery Lancet,1 and are summarized below.
Study design and baseline characteristics1
- Patients with previously untreated high-risk AML/s-AML aged 60–75 years of age were randomized 1:1 to receive CPX-351 (n = 153) or 7+3 (n = 156).
- Patients received 1–2 induction cycles (Figure 1) and 1–2 consolidation cycles were received by those in either complete remission (CR) or CR with incomplete neutrophil or platelet recovery (CRi).
- Baseline patient characteristics were well matched across both groups (Table 1)
s-AML, secondary acute myeloid leukemia.
Table 1. Baseline patient characteristics
|
AML, acute myeloid leukemia; BM, bone marrow; CMML, chronic myelomonocytic leukemia; ECOG PS, Eastern Cooperative Oncology Group performance status; HMA, hypomethylating agent; MDS, myelodysplastic syndrome; NCCN, National Comprehensive Cancer Network; t-AML, therapy-related AML; WBC, white blood cell. |
||
|
Characteristic |
CPX-351 (n = 153) |
7+3 (n = 156) |
|---|---|---|
|
Age, % |
||
|
60–69 years |
63 |
65 |
|
Male/female, % |
61/39 |
62/38 |
|
ECOG PS, % |
||
|
0 |
24 |
29 |
|
AML subtype, % |
||
|
t-AML |
20 |
21 |
|
Prior HMA therapy, % |
41 |
46 |
|
Cytogenetic risk by NCCN, % |
|
|
|
Favorable |
5 |
3 |
|
Median BM blasts, % |
35 |
35 |
|
WBC count < 20,000/µL, % |
86 |
85 |
Results1
- With a median follow-up of 60.65 months, the median overall survival (OS) was 9.33 months for CPX-351 vs 5.95 months for 7+3 (HR, 0.70; 95% CI, 0.55–0.91), which was very stable and consistent with the previous analysis.
- 5-year estimated Kaplan-Meier (KM) survival rate was higher for CPX-351 compared with 7+3 (18% vs 8%, respectively).
- A multivariable cox regression analysis revealed that lower Eastern Cooperative Oncology Group (ECOG) performance status, non-poor karyotype, higher white blood cell count, and lower platelet count were also associated with a longer OS (Table 2).
Table 2. Multivariable analysis of baseline factors associated with OS1
|
CI, confidence interval; ECOG PS, Eastern Cooperative Oncology Group performance status; HR, hazard ratio; OS, overall survival; WBC, white blood cell. |
||
|
Factor |
% of patients |
HR (95% CI) |
|---|---|---|
|
ECOG PS |
|
|
|
0 |
25 |
0.53 (0.33–0.84) |
|
Karyotype |
|
|
|
Non-poor |
46 |
0.49 (0.36–066) |
|
WBC count |
|
|
|
< 20 × 109/L |
61 |
1.64 (1.25–2.16) |
|
Platelet count |
|
|
|
≥ 50 × 109/L |
86 |
0.64 (0.44–0.93) |
|
Treatment arm |
|
|
|
CPX-351 |
50 |
0.70 (0.53–0.92) |
- Improved OS and estimated KM survival rates were maintained at 5 years, regardless of age subgroup (Table 3).
Table 3. Survival data by age subgroup1
|
CI, confidence interval; HR, hazard ratio; KM, Kaplan-Meier; mOS, median overall survival; SR, survival rate; yr, year. |
|||||
|
Age subgroup |
Treatment |
mOS, |
HR (95% CI) |
3-yr KM-estimated SR, % |
5-yr KM-estimated SR, % |
|---|---|---|---|---|---|
|
60–69 yrs |
CPX-351 |
9.59 |
0.73 (0.54–0.99) |
23 |
20 |
|
70–75 yrs |
CPX-351 |
8.87 |
0.52 (0.34–0.77) |
18 |
16 |
- 35% of patients in the CPX-351 arm and 25% in the 7+3 arm went on to receive a hematopoietic stem cell transplant (HSCT).
- Of these patients, the estimated 3-year and 5-year survival rate from the time of transplant was > 50% in the CPX-351 arm (approximately double that of the 7+3 arm).
- The median OS was not yet reached for the CPX-351 arm and 10.35 months for the 7+3 arm (HR, 0.51; 95% CI, 0.28–0.90).
- 48% and 33% of patients achieved CR/CRi in the CPX-351 and 7+3 arms, respectively.
- Of these patients, the median OS was longer for CPX-351 compared with 7+3 (21.72 vs 10.41 months), with a higher estimated survival rate at 3 years (36% vs 23%) and 5 years (30% vs 19%).
- 56% of these patients in the CPX-351 arm and 46% in the 7+3 arm subsequently underwent HSCT. The median OS from the time of transplant was also not yet reached with CPX-351, and was 11.65 months with 7+3 (HR, 0.59; 95% CI, 0.26–0.97).
- The causes of death were similar between both arms, with the most common cause of death being progressive leukemia (CPX-351 arm: 56% and 7+3 arm: 53%).
- 30-day mortality was lower in the CPX-351 arm compared with the 7+3 arm (6% vs 11%).
- 60-day mortality was also lower in the CPX-351 arm compared with the 7+3 arm (14% vs 21%).
Conclusion
These final 5-year follow-up results demonstrate that the improved OS with CPX-351 compared with 7+3 is maintained, regardless of age subgroup, among patients who achieved a CR/CRi, and in those who underwent HSCT. Thus, these data suggest deeper responses can be achieved with CPX-351 than conventional 7+3 and support the prior evidence that CPX-351 contributes to long-term remission and survival in older patients with newly diagnosed high-risk AML or s-AML.
Limitations to this phase III trial are that it only included patients that were 60–75 years of age and excluded those with a creatinine of ≥ 2 mg/dL or with ECOG performance status ≥ 3. Moreover, only ~45% of patients had received prior hypomethylating agent therapy. Therefore, a proportion of ‘unfit’ and elderly patients were not included in the trial. However, a single center, dose expansion, phase II trial (NCT02286726) has been designed to include these patients (25% of patients were ≥ 75 years of age and 82% had prior exposure to hypomethylating agents). This trial also analyzed the effect of dosage on efficacy and safety in this patient population. The results were published in the journal Leukemia2 and demonstrated that higher doses of CPX-351 did not have a noticeable impact on safety and were more efficacious, with 44% of patients reaching a CR/CRi in the 100 mg/m2 dose group. The median OS for this dose group was 6.2 months, which appears favorable with other treatment options for this patient population.
When analyzed together, these results demonstrate that CPX-351 is safe and efficacious for patients considered to be at a high risk of induction mortality with intensive chemotherapy.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?