All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Clinical characteristics and outcomes of patients with AML with inv(3)(q21q26.2)/t(3;3)(q21;q26.2)
Do you know... In a retrospective study on patients with NPM1-mutated R/R AML, which of the following types of treatment yielded the highest response rates, leading to improved relapse-free survival and overall survival rates?
Inv(3)(q21q26.2) and t(3;3)(q21;q26.2) are types of chromosomal abnormalities present in ~1% of patients with newly diagnosed (ND) acute myeloid leukemia (AML) and are associated with dismal outcomes.1 The 2022 European LeukemiaNet (ELN) guidelines classify the presence of inv(3)(q21q26.2)/t(3;3)(q21;q26.2) as an adverse risk. Patients with AML with inv(3)(q21q26.2) and t(3;3)(q21;q26.2) frequently have additional chromosomal abnormalities, the most common being monosomy 7. There is a need to understand how the clinicopathological characteristics of AML with inv(3)(q21q26.2)/t(3;3)(q21;q26.2) affect prognosis and treatment and the potential benefit of allogeneic hematopoietic stem cell transplantation (allo-HSCT) in this patient group.1
Here, we summarize a retrospective study, published by Richard-Carpentier et al.1 in Haematologica, on the clinicopathological characteristics of patients with AML with inv(3)(q21q26.2) or t(3;3)(q21;q26.2) and their impact on clinical outcomes.
Study design and patient characteristics
This retrospective cohort study identified the presence of inv(3)(q21q26.2) or t(3;3)(q21;q26.2) in patients diagnosed with AML at the MD Anderson Cancer Center from January 2000 to September 2020. A total of 108 patients with AML with inv(3)(q21q26.2)/t(3;3)(q21;q26.2) were included; 53 patients and 55 patients were in the ND AML and relapsed/refractory (R/R) cohorts, respectively (Table 1).
Table 1. Baseline characteristics*
|
ACA, additional chromosomal abnormalities; AML, acute myeloid leukemia; BM, bone marrow; CK, complex karyotype; del, deletion; Hb, hemoglobin; inv, inversion; MK, monosomal karyotype; ND, newly diagnosed; PB, peripheral blood; R/R, relapsed/refractory; t, translocation; t-AML, therapy-related AML; WBC, white blood cell. |
||||
|
Characteristics, % (unless otherwise specified) |
Total |
ND AML cohort |
R/R AML cohort |
p value |
|---|---|---|---|---|
|
Median age (range), years |
55 (16–84) |
63 (16–84) |
48 (18–83) |
<0.01 |
|
Age ≥60 years |
41 |
53 |
30 |
0.01 |
|
Male |
63 |
58 |
67 |
0.46 |
|
Median WBC (range), × 109/L |
3.9 (0.3–143.2) |
4.1 (0.6–143.2) |
3.4 (0.3–101.0) |
0.06 |
|
Hb (range), g/dL |
8.8 (5.7–17.1) |
8.6 (5.7–17.1) |
8.9 (7.0–13.8) |
0.81 |
|
Platelets (range), × 109/L |
67 (7–787) |
80 (15–787) |
50 (7–372) |
0.02 |
|
Median PB blasts (range) |
20 (0–96) |
18 (0–96) |
21 (0–93) |
0.34 |
|
Median BM blasts (range) |
48 (16–94) |
35 (16–94) |
54 (19–92) |
0.02 |
|
Secondary AML |
27 |
21 |
33 |
0.24 |
|
t-AML |
18 |
32 |
5 |
<0.01 |
|
inv(3)(q21q26.2) |
81 |
85 |
76 |
0.38 |
|
ACA |
77 |
72 |
82 |
0.31 |
|
−7/del(7q) |
56 |
53 |
58 |
0.71 |
|
del(5q) |
16 |
17 |
15 |
0.93 |
|
CK† |
30 |
25 |
35 |
0.35 |
|
MK‡ |
49 |
47 |
51 |
0.84 |
Key findings
Genetic characteristics
AML with inv(3)(q21q26.2) was identified in 81% of patients. However, only patients with AML with inv(3)(q26.2;q21) showed a white blood cell (WBC) count ≥20 × 109/L (25% vs 0%; p = 0.02).
Mutated genes
- The most frequently mutated gene in this population was SF3B1 (Figure 1).
- NRAS mutations were associated with more frequent occurrence of WBC count ≥20 × 109/L (39% vs 14%; p = 0.02).
- NRAS mutations were also more common in the R/R AML versus ND AML cohort (14% ND vs 33% R/R; p = 0.04).
- KRAS mutations were associated with a higher median peripheral blood blast (PBB) percentage (52% vs 16%; p < 0.01).
- TP53 mutations occurred more frequently in the ND AML compared with the R/R AML cohort (16% vs 0%; p = 0.04).
- ASXL1 and NRAS mutations were reported more often in patients with secondary AML (ASXL, 33% vs 6%; p = 0.046 and NRAS, 46% vs 16%; p < 0.01).
Figure 1. Frequency of gene mutations in patients with AML with inv(3)(q21q26.2)/t(3;3)(q21;q26.2)*
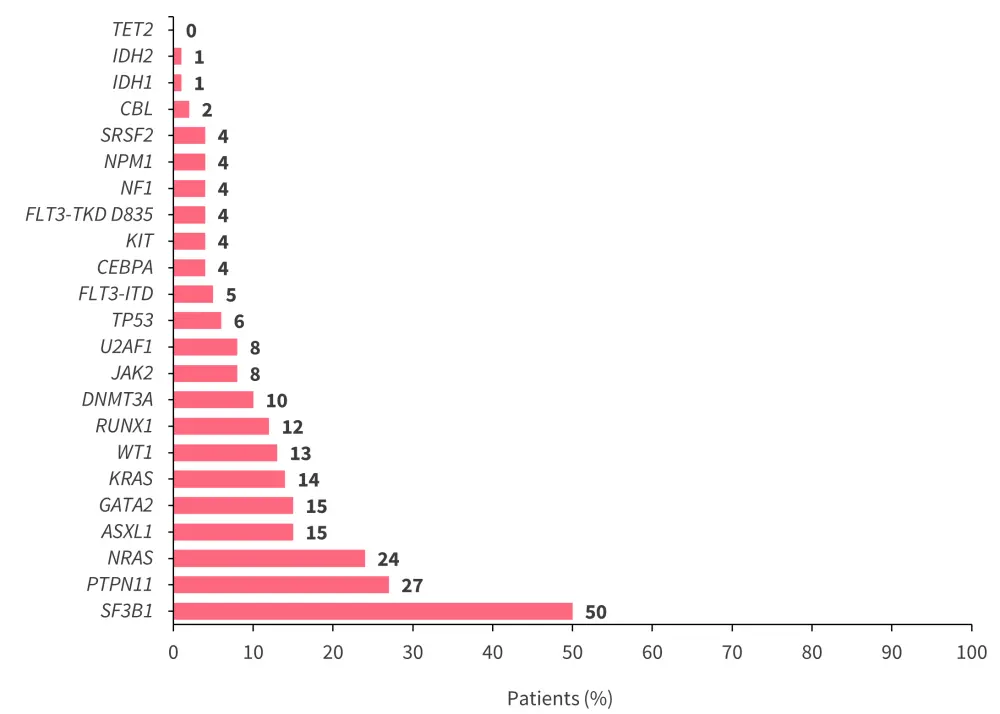
AML, acute myeloid leukemia; inv, inversion; t, translocation.
*Adapted from Richard-Carpentier, et al.1
Remission rates
In total, 96 patients who received treatment were evaluable for response. Composite complete remission (CRc) was achieved by 46% vs 14% (p < 0.01) of patients in the ND AML and R/R AML cohorts, respectively (Table 2). The rate of measurable residual disease negativity was 38% vs 0% in the ND AML and R/R AML cohorts, respectively. The median duration of CRc was 5.4 months in patients who received venetoclax-based regimens.
ND AML cohort
- CRc rates were similar for patients treated with high- and low-intensity treatments (p = 1.00).
- The 30-day mortality rates were comparable between high- and low-intensity treatment groups (p = 0.16).
- In the univariate analyses, higher PBB percentage was associated with lower CRc in the ND AML cohort (odds ratio, 0.98; p = 0.02).
- Lower CRc rates were observed in patients with secondary AML versus patients with ND AML (10% vs 38%; p = 0.02).
R/R AML cohort
- CRc rates were not significantly different between patients who received high- and low-intensity treatments (p = 0.39).
- The 30-day mortality rates were similar between the high- and low-intensity treatment groups (p = 1.00).
Table 2. Response rates*
|
AML, acute myeloid leukemia; CR, complete remission; CRc, composite CR; CRi, CR with incomplete hematological recovery; HI, high intensity; HMA, hypomethylating agents; LI, low intensity; MLFS, morphologic leukemia-free state; ND, newly diagnosed; ORR, overall response rate; R/R, relapsed/refractory; Ven, venetoclax. †An additional patient treated with a low-intensive venetoclax-based regimen achieved MLFS and is not included in the CRc rates. |
||||||||
|
Clinical outcome, % (unless otherwise specified) |
Total |
ND AML cohort |
R/R AML cohort |
|||||
|---|---|---|---|---|---|---|---|---|
|
Total |
HI |
LI |
Total |
HI |
LI |
|||
|
CRc |
31 |
46 |
46 |
47 |
14 |
20 |
8 |
|
|
CR |
17 |
29 |
26 |
35 |
2 |
5 |
0 |
|
|
CRi |
15 |
17 |
20 |
12 |
11 |
15 |
8 |
|
|
MLFS |
2 |
4 |
0 |
12 |
0 |
0 |
0 |
|
|
ORR |
33 |
50 |
46 |
59 |
14 |
20 |
8 |
|
|
No. of cycles to remission (range) |
1 (1–4) |
1 (1–4) |
1 (1–2) |
1.5 (1–4) |
1.5 (1–3) |
1.5 (1–3) |
1.5 (1–2) |
|
|
Median days to remission (range) |
39.5 (19–126) |
37 (19–126) |
34.5 (20–85) |
53 (19–126) |
53.5 (27–102) |
73 (31–102) |
42 (27–57) |
|
|
30-day mortality |
8 |
10 |
14 |
0 |
7 |
5 |
8 |
|
|
CRc according to treatment type |
|
|
|
|
|
|
|
|
|
With Ven |
33† |
20† |
0 |
25† |
43 |
66 |
24 |
|
|
Without Ven |
31 |
49 |
47 |
54 |
8 |
12 |
5 |
|
|
With HMA |
36 |
50 |
NA |
50 |
20 |
NA |
20 |
|
|
Without HMA |
10† |
40† |
NA |
40† |
0 |
NA |
0 |
|
Survival outcomes
- At a median follow-up of 83 months, the median overall survival (OS) was 7.9 months and 5.9 months in the ND AML and R/R AML cohorts, respectively.
- The 3-year OS rate was 8.8% vs 7.1% in the ND AML and R/R AML cohorts, respectively.
- The median relapse-free survival (RFS) was 4.1 months, with a 3-year RFS rate of 8.6% and a 3-year cumulative incidence of relapse rate of 81.7%.
- In total, 6% of patients were alive at the last follow up or had RFS ≥5 years.
- Univariate analyses revealed that age (hazard ratio [HR], 1.01; p = 0.04), WBC count ≥20 × 109/L at diagnosis (HR, 1.02; p < 0.01), higher PBB percentage (HR, 1.01; p < 0.01), and secondary AML (HR, 1.81; p = 0.01) were associated with worse OS.
- A WBC count ≥20 × 109/L was associated with significantly worse OS compared with a WBC count ≤20 x 109/L (HR, 2.19; p < 0.01).
- Multivariable analyses revealed that higher WBC count ≥20 × 109/L (HR, 5.67; p < 0.01), secondary AML (HR, 4.14, p < 0.01), and ASXL1 mutations (HR, 2.83; p = 0.049) were independently associated with worse OS.
- Mutation analysis revealed the following:
- NRAS mutations were associated with inferior OS (HR, 2.39; p = 0.06) among patients in the ND AML cohort.
- KRAS mutation was associated with poor OS (HR, 2.37; p = 0.01), particularly in the R/R AML cohort.
- ASXL1 (HR, 2.62; p = 0.04) and DNMT3A (HR, 3.09; p = 0.02) mutations were also associated with poor OS.
Allo-HSCT
- Among patients achieving CRc or morphologic leukemia-free state, 31% received allo-HSCT in first complete remission (CR1).
- The median time from response to allo-HSCT was 56 days and 39 days in the ND AML and R/R AML cohorts, respectively.
- At 4 months, allo-HSCT in CR1 was associated with improved OS (HR, 0.33; p = 0.03).
- The 5-year OS rates were higher in patients who received allo-HSCT compared with those who did not receive allo-HSCT in CR1 (44% vs 6%).
- The 2-year cumulative incidence of relapse was lower among patients who received allo-HSCT compared with those who did not receive allo-HSCT in CR1 (57% vs 86%).
- Time-dependent variable analysis showed allo-HSCT in CR1 improved RFS (HR, 0.39; p = 0.046) and generally showed a trend towards improving OS (HR, 0.41; p = 0.08).
Conclusion
This retrospective study highlights the very poor prognosis associated with AML with inv(3)(q21q26.2)/t(3;3)(q21;q26.2). Current treatment options for this patient population remain limited, with similar response rates observed in both high- and low-intensity chemotherapy treatment groups in the ND AML cohort. The addition of venetoclax did not improve response rates, suggesting that hypomethylating agent-based therapies may be the preferred treatment option in this patient group. While allo-HSCT in CR1 was associated with improved survival outcomes, few patients in this study proceeded to transplantation due to high rates of relapse. This study demonstrates the need for novel therapeutics to treat patients with inv(3)(q21q26.2)/t(3;3)(q21;q26.2).
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?
