All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
ASCO22 Annual Meeting roundup – Ivosidenib
Isocitrate dehydrogenase-1 (IDH1) mutations are present in 6–10% of cases of acute myeloid leukemia (AML) and are associated with oncogenesis. Recent research has investigated the role of the potent oral IDH1 inhibitor ivosidenib (Ivo), particularly in patients who are ineligible for intensive chemotherapy. Below we summarize three poster presentations from the 2022 American Society of Clinical Oncology (ASCO) Annual Meeting, which covered safety data on Ivo + venetoclax (Ven) with or without azacitidine (Aza) in IDH1-mutated hematologic malignancies, as well as further analysis of the phase III AGILE trial, supporting the U.S. Food and Drug Administration (FDA) approval of Ivo + Aza.
Ivo + Ven with or without Aza – A phase I/II study1
Curtis Andrew Lachowiez et al.1 investigated a combination of Ivo + Ven in 31 patients across four dosing levels (Figure 1).
Figure 1. Study design*
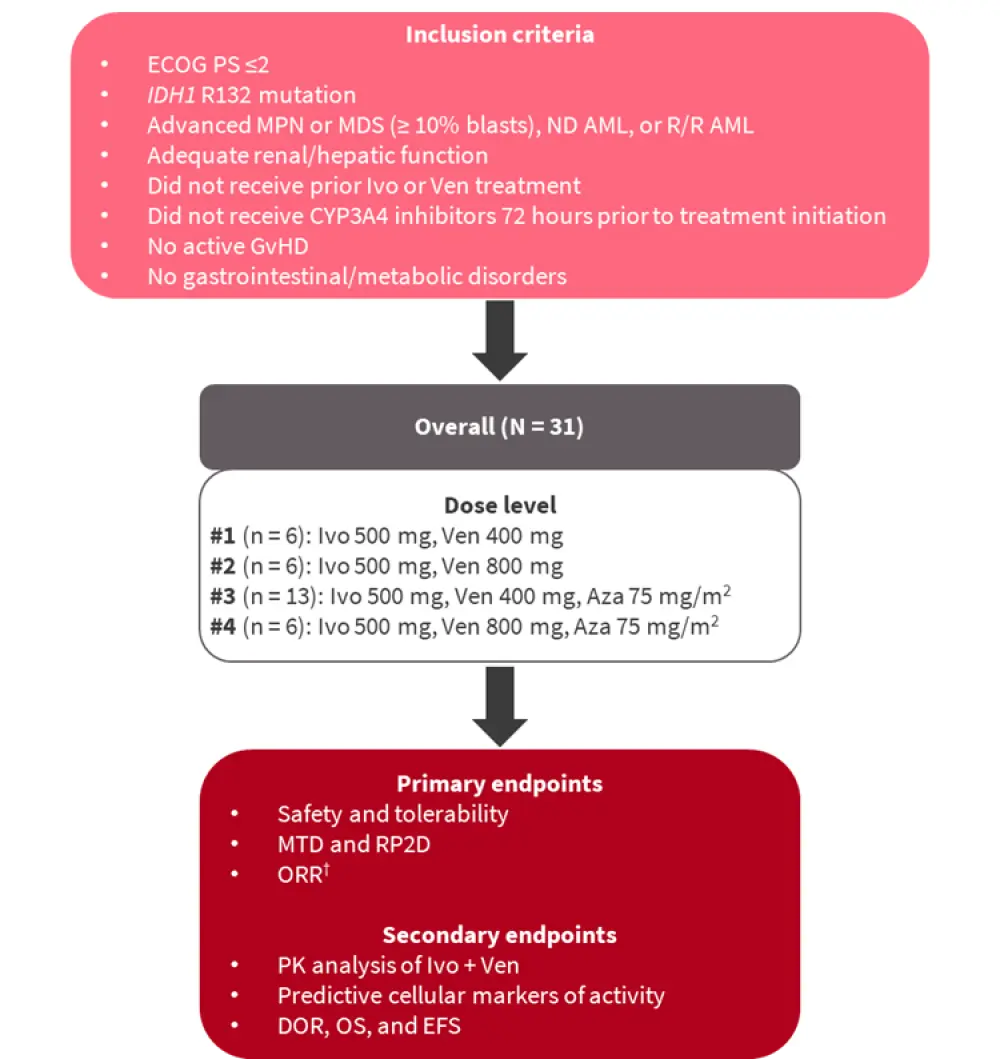
AML, acute myeloid leukemia; Aza, azacitidine; DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group performance score; EFS, event-free survival; GvHD, graft-versus-host disease; Ivo, ivosidenib; MDS, myelodysplastic syndromes; MPN, myeloproliferative neoplasms; MTD, median tolerated dose; ND, newly diagnosed; ORR, overall response rate; OS, overall survival; PK, pharmacokinetic; RP2D, recommended phase II dose; R/R, relapsed/refractory; Ven, venetoclax.
*Adapted from Lachowiez et al.1
†ORR includes complete response (CR) + complete response with incomplete count recovery (CRi) + complete response with incomplete hematologic recovery (CRh) + partial response (PR) + morphological leukemia-free state (MLFS).
Patient characteristics are summarized in Table 1. Almost half of all patients (48%) received prior treatment. Two-thirds of the cohort had AML, and over half of patients had adverse cytogenetics using the European LeukemiaNet (ELN) 2017 criteria.
Table 1. Patient characteristics*
|
AML, acute myeloid leukemia; BM, bone marrow; ECOG PS, Eastern Cooperative Oncology Group performance score; ELN, European LeukemiaNet; MDS, myelodysplastic syndromes; MPN, myeloproliferative neoplasms; ND, newly diagnosed; R/R, relapsed/refractory. |
|
|
Characteristic |
N = 31 |
|---|---|
|
Median age, years (range) |
67 (44–84) |
|
Male, % |
65 |
|
Median baseline BM blasts, % (range) |
23 (1–80) |
|
ECOG PS, % |
|
|
0 |
27 |
|
1 |
60 |
|
2 |
13 |
|
Disease type, % |
|
|
MDS/MPN |
29 |
|
ND-AML |
45 |
|
R/R AML |
26 |
|
2017 ELN risk group |
|
|
Favorable |
26 |
|
Intermediate |
19 |
|
Adverse |
55 |
|
Received prior treatment, % |
48 |
Results
Safety and tolerability
- Safety and tolerability outcomes were as expected, with febrile neutropenia observed in nine (29%) patients, eight of whom experienced Grade 3 events, and one Grade 5 events
- Lung infection occurred in 19% of patients
- One patient died secondary to febrile neutropenia
- Regarding adverse events of special interest, tumor lysis syndrome (TLS) occurred in two patients, one of whom experienced spontaneous TLS with treatment initiation (onset, Day 0), and one of these events was a dose-limiting toxicity (DLT)
- IDH-differentiation syndrome was observed in four patients, with a median onset of 39 days, and no DLTs occurred
- No 30- or 60-day mortality was observed
Efficacy
- The overall response rate (ORR) was 67% at dose level 1 (DL1) and 100% at DL2, DL3, and DL4
- At DL3, partial remission as well as morphologic leukemia-free state, were included in the ORR, with a composite complete remission (CRc) rate of 85%
- For patients who received ≥5 cycles of therapy, 64% achieved IDH1 mutation clearance, indicating a deepened response over time
- When considering both DLs and disease type, there was no significant difference in median overall survival (OS) (median OS, 26 months for DL1, and not reached for all other DLs)
- Median event-free survival (EFS) was 7.9 months at DL1, 8.7 months at DL2, and not reached for DL3 and DL4
- Median OS was 42.1 months for myelodysplastic syndromes/myeloproliferative neoplasms (MDS/MPN), and not reached for both newly diagnosed and relapsed/refractory (R/R) AML
- Detection of IDH1 mutations by digital droplet polymerase chain reaction (PCR) was not predictive of OS, but the multi-color flow cytometry detection of minimal residual disease (MRD) positivity was associated with a reduced OS (p = 0.0015)
In summary, Ivo + Ven with and without azacitidine resulted in deep responses across several hematologic malignancies, with an expected and tolerable safety profile. Responses appeared to deepen over time, with the majority of patients who received ≥5 treatment cycles achieving IDH1-mutated clone clearance.
Molecular characterization of Ivo + Aza response2
Botton et al.2 presented findings from the AGILE study (NCT03173248), in which 500 mg Ivo + 75 mg/m2 Aza was compared with placebo + Aza in patients with newly diagnosed IDH1-mutated AML who were ineligible for intensive chemotherapy. We previously summarized key efficacy and safety findings from this trial in a visual abstract. Botton et al.2 presented the molecular analysis of bone marrow and peripheral blood mononuclear cells, as of the March 18, 2021 data cutoff, as well as the IDH1 mutation clearance analysis using BEAMing digital PCR, and a co-mutation analysis using next-generation sequencing (NGS).
Results
- The combination of Ivo + Aza (43 patients) led to improved clearance of the IDH1 mutation, and less recurrence of the IDH1 mutation, when compared with Aza + placebo (34 patients)
- In patients achieving complete response (CR)/complete response with incomplete hematologic recovery (CRh), suppression of mutant IDH1 was more durable with Ivo + Aza treatment (clearance maintained in 17/17 patients) versus placebo (clearance maintained in 1/3 patients).
- Analysis of 58 patients receiving Ivo + Aza and 62 patients receiving Aza + placebo revealed DNMT3A, SRSF2, and RUNX1 as the most commonly co-mutated genes in both cohorts
- Mutations in DNMT3A, RUNX1, SRSF2, and RTK pathways were associated with improved outcomes in patients treated with Ivo + Aza (Figure 2).
- The RTK pathway has previously been noted to be associated with primary resistance to Ivo monotherapy.
Figure 2. CR + CRh based on baseline mutation status*
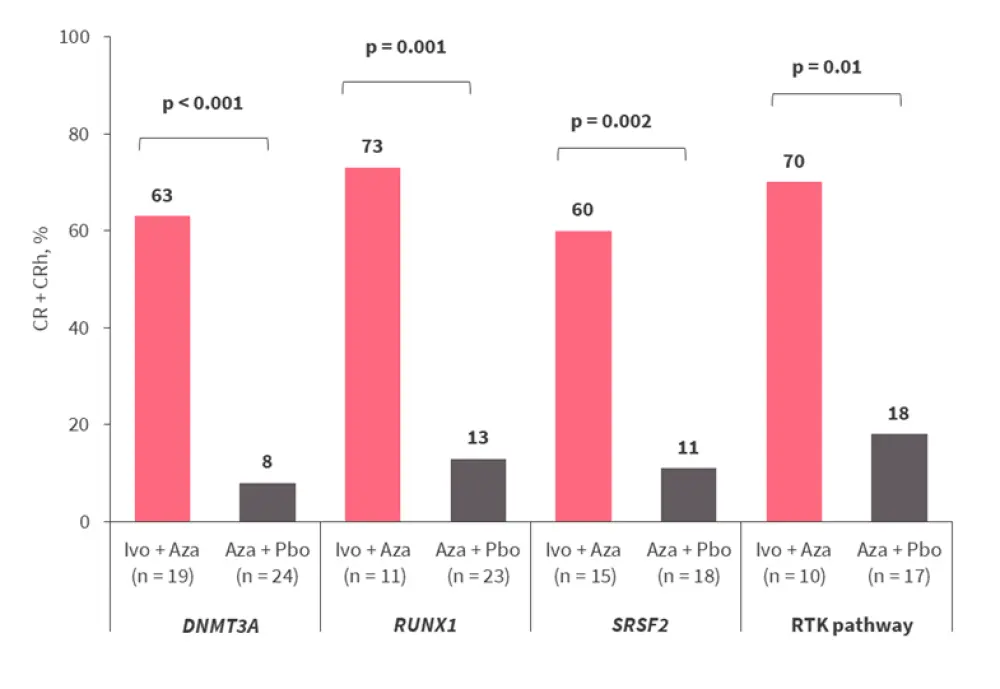
Aza, azacitidine; CR, complete remission; CRh, complete remission with incomplete hematologic recovery; Ivo, ivosidenib; Pbo, placebo.
*Adapted from Botton et al.2
In summary, molecular analysis of data from the AGILE trial demonstrated improved IDH1 mutation clearance and deeper responses with Ivo + Aza versus Aza + placebo. Mutations in the DNMT3A, RUNX1, SRSF2, and RTK pathways were associated with improved CR/CRh; further investigations are necessary to determine if the combination Ivo + Aza overcomes the resistance to Ivo alone previously noted with the RTK pathway.
Hematologic improvements of Ivo + Aza vs Aza + placebo3
Hartmut Döhner presented further results from the AGILE trial, where rates of blood count recovery and transfusion independence were assessed in patients receiving Ivo + Aza versus Aza + placebo.
Blood count recovery
- Ivo + Aza led to a rapid increase in median absolute neutrophil count (baseline, 0.99 × 109/L; Week 2, 2.05 × 109/L; Week 5, 4.07 × 109/L), and stabilized to within normal range by the end of the study
- In the placebo arm, the mean neutrophil counts initially declined before recovering to normal levels at 36–40 weeks
- Increased blood counts were accompanied by a decrease in bone marrow (BM) blast percentage, which was more rapid in the Ivo + Aza arm (baseline, 54.8%; Week 9, 12.0%; Week 17, 7.2%)
- Decreases in BM blast percentage were slower in the placebo arm (baseline, 53.7%; Week 9, 34.6%; Week 17, 19.6%)
- Median hemoglobin level steadily increased from baseline at a similar rate in both treatment arms
- Mean absolute platelet count (109/L) also steadily increased in both treatment arms, and stabilised around 24 weeks
Transfusion independence
- Rates of transfusion independence were higher in the Ivo + Aza cohort compared with the Aza + placebo cohort (46.2% vs 17.5%) for patients who were transfusion-dependent at baseline
- A total of 69.7% of patients maintained transfusion independence in the Ivo + Aza arms vs 61.8% in the placebo arm
In summary, these results demonstrated faster recovery of blood counts with Ivo + Aza vs Aza + placebo, and improved rates of transfusion independence.
Conclusion
These novel data confirm the potential of Ivo in IDH1-mutated AML, in doublet combination with Aza, and as a triplet with Ven.1 Further analysis of the AGILE trial revealed benefits on blood count recoveries and transfusion independence,3 and molecular evaluation found specific mutations which may particularly benefit from these therapies.2
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?