All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Kura Oncology, Syndax, Abbvie, Thermo Fisher and Johnson & Johnson. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Venetoclax-based combination therapies for AML in patients ineligible for intensive chemotherapy
Do you know... Which of the following treatments is most likely to have a survival benefit for treatment-naïve patients with AML who are ineligible for intensive chemotherapy?
Treatment for patients with acute myeloid leukemia (AML) typically consists of intensive chemotherapy; however, many patients are ineligible for intensive chemotherapy due to toxicity.1 Treatment in these patients typically includes lower-intensity regimens, such as hypomethylating agents, low-dose cytarabine, or supportive care.
The use of venetoclax, a B-cell lymphoma 2 inhibitor has been extensively covered by the AML Hub. In addition, the VIALE-A (NCT02993523) and VIALE-C (NCT03069352) trials have demonstrated the efficacy of venetoclax in combination with azacitidine or low-dose cytarabine, respectively, in patients with AML who are ineligible for intensive chemotherapy.1
To date, there have been no head-to-head randomized controlled trials comparing the efficacy of venetoclax-based combinations with conventional treatment options in patients with AML who are ineligible for intensive chemotherapy.1 Li et al. recently published a network meta-analysis assessing the efficacy of venetoclax-based combinations compared with conventional treatment options in Value Health. Here, we summarize the key points.
Methods1
In October 2020, a systematic literature review was performed to identify phase III randomized controlled trials for network meta-analyses. Eligible trials compared complete remission (CR) + CR with incomplete count recovery (CRi) and overall survival (OS) for ≥2 treatments of interest in adult patients with AML who were ineligible for intensive chemotherapy.
Two separate network meta-analyses were conducted for CR + CRi and OS. Relative rankings for each treatment were estimated based on surface area under the cumulative ranking curve (SUCRA) value, with a higher SUCRA indicating the treatment was more likely to be efficacious in the network.
In total, five randomized controlled trials were included in this analysis (Figure 1).
Figure 1. Randomized controlled trials included in the venetoclax network meta-analysis*
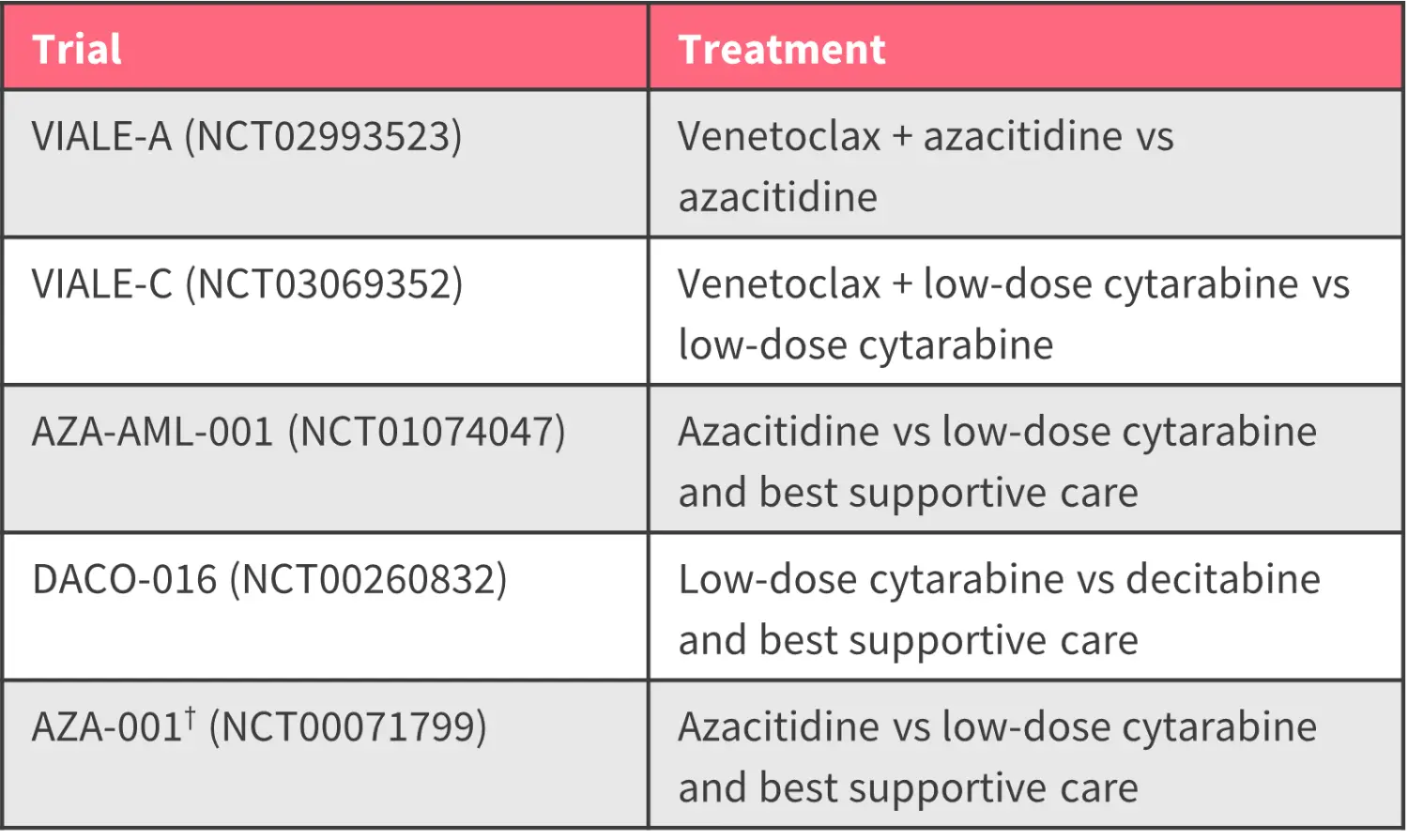
CR, complete remission; CRi, CR with incomplete count recovery.
*Data from Li et al.1
†The AZA-001 trial was not included in the CR + CRi analysis.
Results1
Responses
Patients treated with venetoclax + azacitidine or venetoclax + low-dose cytarabine were more likely to achieve CR + CRi than patients receiving azacitidine, low-dose cytarabine, or best supportive care (Table 1). Patients who received venetoclax-based combinations were numerically more likely to achieve CR + CRi than patients treated with decitabine, but this did not reach statistical significance.
Table 1. Pairwise treatment comparison of CR + CRi*
|
AZA, azacitidine; BSC, best supportive care; CR, complete remission; CRi, CR with incomplete count recovery; DEC, decitabine; LDAC, low-dose cytarabine; VEN, venetoclax. |
|
|
Odds ratio, n (95% credible interval) |
VEN + AZA |
|---|---|
|
VEN + LDAC |
0.90 (0.31–2.42) |
|
AZA |
5.06† (3.31–7.97) |
|
LDAC |
5.74† (3.01–11.35) |
|
DEC |
2.07 (0.90–4.80) |
|
BSC |
20.68† (5.63–104.99) |
|
VEN + LDAC |
|
|
AZA |
5.64† (2.33–14.97) |
|
LDAC |
6.39† (3.10–14.76) |
|
DEC |
2.30 (0.94–6.06) |
|
BSC |
23.28† (5.63–135.69) |
|
AZA |
|
|
LDAC |
1.14 (0.70–1.85) |
|
DEC |
0.41† (0.20–0.83) |
|
BSC |
4.08† (1.22–19.61) |
|
LDAC |
|
|
DEC |
0.36† (0.21–0.59) |
|
BSC |
3.57† (1.08–17.57) |
|
DEC |
|
|
BSC |
9.96† (2.89–50.74) |
Based on cumulative treatment rankings, venetoclax-based combinations were the highest-ranked, followed by decitabine, azacitidine, low-dose cytarabine, and best supportive care (Figure 2).
Figure 2. SUCRA values for CR + CRi*
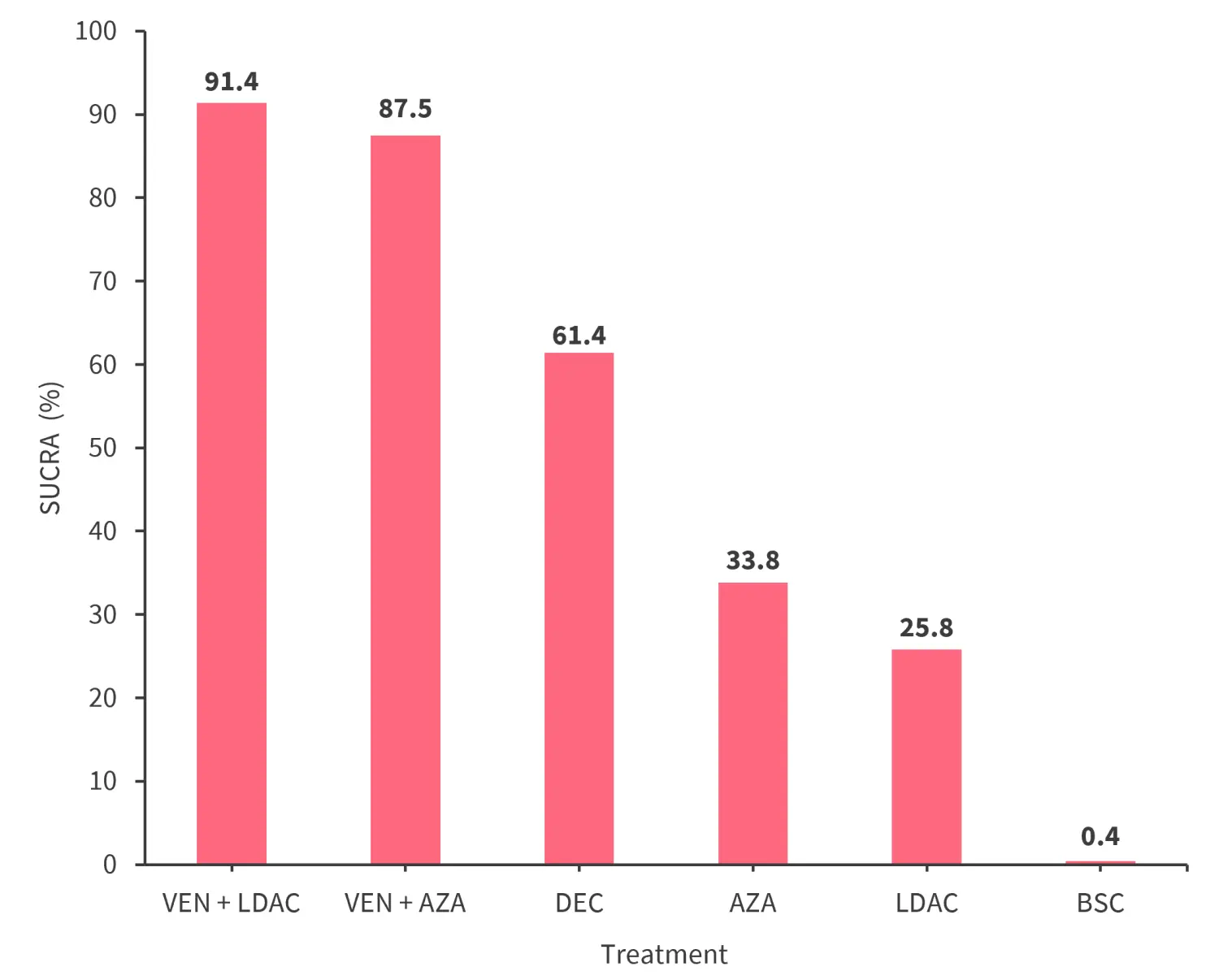
AZA, azacitidine; BSC, best supportive care; CR, complete remission; CRi, CR with incomplete count recovery; DEC, decitabine; LDAC, low-dose cytarabine; SUCRA, surface area under the cumulative ranking curve; VEN, venetoclax.
*Data from Li, et al.1
Survival
Patients treated with venetoclax + azacitidine had a lower risk of death compared with patients treated with azacitidine, low-dose cytarabine, and best supportive care (Table 2). Treatment with venetoclax + low-dose cytarabine was also associated with a lower risk of death compared with low-dose cytarabine + best supportive care (Table 2). Patients treated had a numerically lower risk of death with venetoclax-based treatment compared with patients treated with decitabine; however, this was not significant.
Table 2. Pairwise treatment comparison of OS*
|
AZA, azacitidine; BSC, best supportive care; DEC, decitabine; LDAC, low-dose cytarabine; OS, overall survival; VEN, venetoclax. |
|
|
Hazard ratio (95% credible interval) |
VEN + AZA |
|---|---|
|
VEN + LDAC |
0.81 (0.50–1.32) |
|
AZA |
0.66† (0.52–0.85) |
|
LDAC |
0.57† (0.41–0.81) |
|
DEC |
0.70 (0.47–1.03) |
|
BSC |
0.37† (0.24–0.59) |
|
VEN + LDAC |
|
|
AZA |
0.81 (0.54–1.24) |
|
LDAC |
0.70† (0.50–0.99) |
|
DEC |
0.86 (0.58–1.26) |
|
BSC |
0.46† (0.26–0.80) |
|
AZA |
|
|
LDAC |
0.86 (0.67–1.10) |
|
DEC |
1.05 (0.77–1.43) |
|
BSC |
0.56† (0.38–0.82) |
|
LDAC |
|
|
DEC |
1.22† (1.01–1.47) |
|
BSC |
0.65 (0.41–1.01) |
|
DEC |
|
|
BSC |
0.53† (0.33–0.86) |
Venetoclax-based treatments were the highest-ranked treatments for OS, followed by decitabine, azacitidine, low-dose cytarabine, and best supportive care (Figure 3).
Figure 3. SUCRA values for OS*
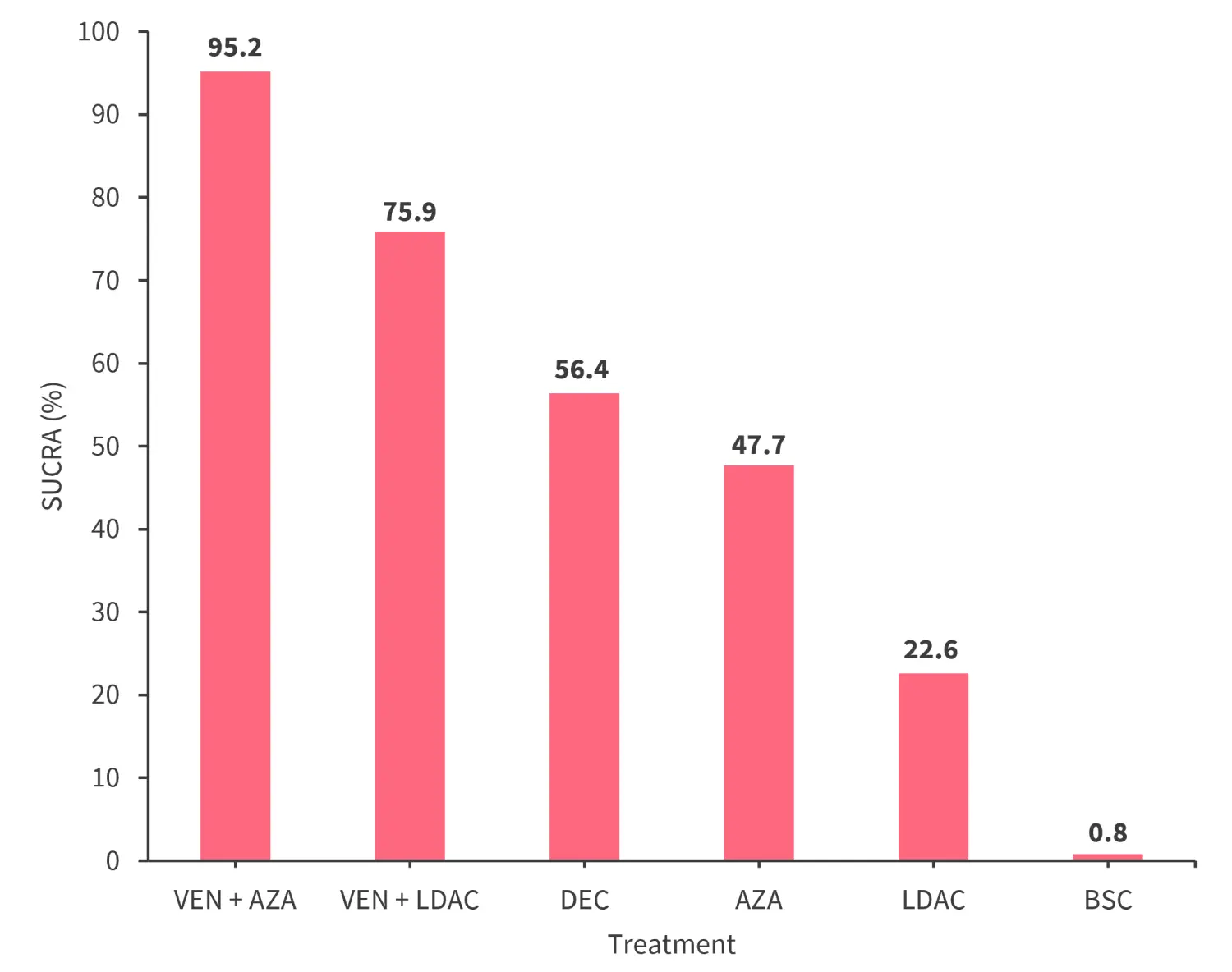
AZA, azacitidine; BSC, best supportive care; DEC, decitabine; LDAC, low-dose cytarabine; OS, overall survival; SUCRA, surface area under the cumulative ranking curve; VEN, venetoclax.
*Data from Li, et al.1
Conclusion
The findings from this analysis suggest that venetoclax-based combinations are associated with improved response rates and survival outcomes when compared with azacitidine, low-dose cytarabine, and best supportive care alone.
While this network meta-analysis provides an indirect comparison of venetoclax-based treatments and other lower-intensity treatments in the absence of phase III randomized controlled trials, there are several limitations; the results may be influenced by the heterogeneity of patient populations across the included trials. Additionally, not all treatment options were captured, particularly venetoclax + decitabine.
Despite these limitations, results suggest that venetoclax-based treatments have the potential to improve outcomes in patients with AML who are ineligible for intensive chemotherapy, a patient population with historically poor outcomes.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the typical turnaround time for next-generation sequencing (NGS) results for AML at your center?

