All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Type I and type II FLT3 inhibitors demonstrate differing patterns of secondary resistance in patients with AML
During the 62nd American Society of Hematology (ASH) Annual Meeting and Exposition, Ahmad Alotaibi presented a retrospective analysis that demonstrated patterns of secondary resistance differ between patients treated with type I and type II FLT3 inhibitors.1 The data were also recently published in the journal Blood Cancer Discovery,2 and are summarized below.
Type I and type II FMS-like tyrosine kinase 3 inhibitors (FLT3i) vary in their ability to bind to active or inactive receptor conformations and different types of FLT3 mutations. Type I FLT3i, such as gilteritinib, midostaurin, and crenolanib, bind to the active receptor conformation and have activity against internal tandem duplication (ITD) and tyrosine kinase domain (TKD) mutations. Whereas type II FLT3i, such as quizartinib, sorafenib, and ponatinib, only bind to the inactive conformation and have no activity against FLT3-TKD mutations.1,2
FLT3i have demonstrated improved survival for patients with FLT3-mutated AML in both the frontline and relapsed/refractory (R/R) setting. Indeed, midostaurin is approved for newly diagnosed patients in combination with standard chemotherapy in the U.S. and Europe. However, the duration of response remains short at 4–14 months and is frequently influenced by the emergence of mutations that drive secondary resistance, including on-target mutations of the TKD, or off-target mutations involved in parallel pro-survival signaling pathways such as RAS-MAPK.1,2
Understanding how mutation profiles change from pre- to post-FLT3i treatment could help with designing strategies to overcome or minimize resistance. Assessing mutational profiles and variant allele frequencies (VAFs) from primary resistance patients against those who respond and then relapse may help the understanding of FLT3i failure and identify patients that would benefit from combinatorial approaches. 1,2
Study design and patient characteristics1,2
- 946 patients with FLT3 mutations were identified from the MD Anderson Cancer Center database between January 2012 and December 2019.
- Of those patients that had available pre- and post-FLT3i next-generation sequencing profiles of their bone marrow,
- 106 patients had no response (primary resistance cohort), and
- 67 patients achieved a composite complete remission (CRc) followed by relapse (secondary resistance cohort).
- Baseline characteristics of the secondary resistance cohort are summarized in Table 1.
- Most patients had de novo AML (78%), and 58% had R/R disease, with a median of two prior therapies (range, 1–5).
- 90% of patients had a FLT3-ITD mutation, 16% a FLT3-D835 mutation, and 6% had both ITD and D835 mutations.
- In the primary resistance cohort, most patients were R/R (92%), with a median of three prior therapies (range, 1–10).
- 85% of patients had a FLT3-ITD mutation, 25% a FLT3-D835, and 10% had both ITD and D835 mutations.
Table 1. Baseline characteristics of the secondary resistance cohort1
|
allo-HSCT, allogenic hematopoietic stem cell transplant; AML, acute myeloid leukemia; FLT3i, FMS-like tyrosine kinase 3 inhibitors; MDS, myelodysplastic syndromes; MPN, myeloproliferative neoplasms; R/R, relapsed/refractory. |
|
|
Characteristics |
n = 67 |
|---|---|
|
Median age, years (range) |
62 (19–85) |
|
Male/female, % |
48/52 |
|
Type of AML, % |
|
|
De novo |
78 |
|
Secondary (post MDS/MPN) |
18 |
|
Therapy related |
4 |
|
Cytogenetics, % |
|
|
Diploid karyotype |
64 |
|
Adverse risk |
21 |
|
Others |
15 |
|
Median no. of mutations at baseline (range) |
4 (1–9) |
|
Frontline patients, % |
42 |
|
R/R patients, % |
58 |
|
Median prior therapies for R/R, n (range) |
2 (1–5) |
|
Prior therapies for R/R, % |
|
|
Intensive chemotherapy |
76 |
|
Allo-HSCT |
18 |
|
FLT3i |
46 |
Results
Details of the therapies received can be seen in Table 2.
- In the secondary resistance cohort, more patients received a type II FLT3i than a type I FLT3i (69% vs 31%).
Table 2. FLT3i treatment for the primary and secondary resistance cohorts1,2
|
Rx, rituximab therapy; FLT3i, FMS-like tyrosine kinase 3 inhibitors. |
||
|
Treatment |
Secondary resistance cohort (n = 67) |
Primary resistance cohort (n = 106) |
|---|---|---|
|
FLT3i + low-intensity Rx, % |
64 |
74 |
|
FLT3i + intensive Rx, % |
33 |
20 |
|
Single agent FLT3i, % |
5 |
26 |
|
Type II FLT3i-based, % |
69 |
54 |
|
Sorafenib, % |
58 |
42 |
|
Quizartinib, % |
11 |
11 |
|
Type I FLT3i-based, % |
31 |
46 |
|
Gilteritinib, % |
18 |
5 |
|
Midostaurin, % |
10 |
12 |
|
Crenolanib, % |
3 |
29 |
In the secondary resistance cohort:1,2
- Complete response (CR) rate was 36%, CR with incomplete platelet recovery (CRp) 25%, and CR with incomplete neutrophil recovery (CRi) 39%.
- Median CRc duration was 4.7 months (95% CI, 3.6–6.1).
- Median overall survival (OS) was 14.1 months (95% CI, 10.5–16.3).
- 31% of patients went on to receive an allogeneic hematopoietic stem cell transplant.
Emergent mutations1,2
- The majority of patients (55%) in the secondary resistance cohort had ≥ 1 emergent mutation at relapse, including 65% of those who received a type II FLT3i and 33% of those who received a type I FLT3i (p = 0.02).
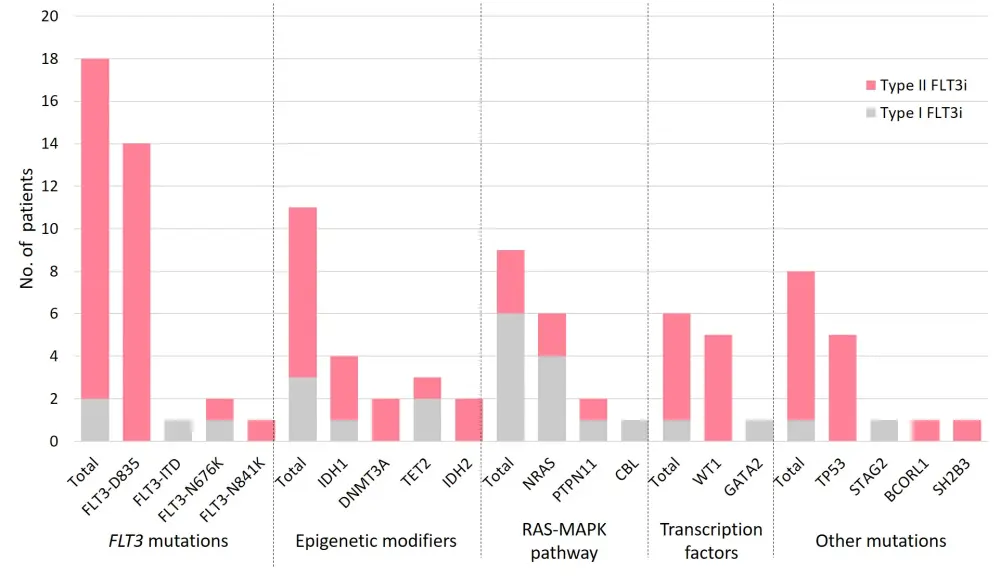
- The most frequent emergent mutations (Figure 1) were FLT3-D835 (21%), RAS/MAPK pathway mutations (13%), IDH1/IDH2 (9%), WT1 (7%), and TP53 (7%).
- The most common emergent mutation for patients treated with type II FLT3i-based therapies was FLT3-D835 (30%).
- The most common emergent mutations for patients treated with type I FLT3i-based therapies were in the RAS/MAPK pathway (29%).
Figure 1. Emergent mutations in the secondary resistance cohort in patients treated with type I/II FLT3 inhibitors (FLT3i)2
Loss of detectable FLT3 mutations at relapse1
- 26% of patients in the secondary resistance cohort no longer had a detectable FLT3 mutation at relapse; this equated to 26% of those treated with type II FLT3i and 28% of those treated with type I FLT3i.
VAF changes from baseline to relapse for the secondary resistance cohort2
- The median VAF of emergent RAS/MAPK mutations increased to 32% from 6% at baseline.
- The median VAF of emergent IDH1, IDH2, and TP53 mutations were lower than the respective median VAFs at baseline.
Outcomes after relapse, with a 15-month follow-up1
- Median OS at relapse was shorter for patients with emergent mutations compared with those without emergent mutations (4.1 months vs 6.7 months; p = 0.31).
- Median OS was significantly better for patients who had an undetectable FLT3 mutation at relapse compared with those with persistent FLT3 mutations (9.9 months vs 4.6 months; p = 0.029).
- For patients that received type II FLT3i-based therapies, the median OS was significantly lower in patients with FLT3-D835 mutations at relapse compared with those without (2.6 months vs 6.7 months; p = 0.002).
- For patients that received type I FLT3i-based therapies, the median OS was significantly lower in patients with emergent RAS/MAPK pathway mutations at relapse compared with those without (2.4 months vs 6.8 months; p = 0.009).
Pretherapy VAF in patients with primary vs secondary resistance2
- The pre-FLT3i VAF of DNMT3A and IDH2 mutations were significantly higher in patients who achieved CRc (secondary resistance cohort) compared with non-responders (primary resistance cohort) (DNMT3A: 54% vs 30%; p = 0.002. IDH2: 21% vs 7%; p = 0.005).
- No significant difference was seen for pre-FLT3i VAF of RAS, PTPN11, IDH1, WT1, or TP53 between those who achieved CRc and non-responders.
Conclusion
The majority of patients that responded to FLT3i and relapsed (secondary resistance) developed treatment-emergent mutations, including on-target mutations in FLT3, and off-target mutations in epigenetic modifiers, RAS/MAPK pathway, WT1, and TP53.
Patients treated with type I or type II FLT3i developed different types of emergent mutation. For those treated with type II FLT3i, FLT3-D835 was the most common emergent mutation, whereas emergent RAS/MAPK pathway mutations were more common for those treated with type I FLT3i. Both types of emergent mutation were also associated with an inferior survival. This suggests leukemic cells may exploit distinct yet potentially predictable secondary pathways of resistance depending on the type of FLT3i used.
There were several limitations to this study. The analysis was comprised of heterogenous FLT3i-based combinations, and therefore the data may not be directly applicable to single-agent based therapies. The next-generation sequencing platform could only detect > 1% mutated alleles, hence small subclones may have been missed pretherapy and may have also expanded post therapy to be detected as an emergent mutation instead of a clonal expansion. Furthermore, the results may reflect a selection bias for patients who had a mutational analysis available, as the original clinical trial designs did not mandate an end-of-treatment mutational analysis.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?