All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Kura Oncology, Syndax, Abbvie, Thermo Fisher and Johnson & Johnson. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Safety and efficacy of flotetuzumab in patients with R/R AML
Limited effective treatment options are available for the treatment of patients with primary induction failure (PIF) or early relapse (ER; relapse after < 6 months) acute myeloid leukemia (AML). In these patients, the response rate to salvage chemotherapy regimens is approximately 12%, and the median overall survival (OS) is 3 months.1
It has been recently reported that an immune-infiltrated tumor microenvironment (TME) with high expression of interferon (IFN)γ-inducible genes can identify patients less likely to respond to cytotoxic chemotherapy but more responsive to immunotherapies, such as flotetuzumab.1
Flotetuzumab is an investigational CD123 × CD3 bispecific antibody. CD123 is highly expressed on the AML blasts of patients who experience PIF/ER, and its expression has been associated with poor outcomes.1 Therefore, flotetuzumab could represent a valid treatment option for patients with PIF/ER AML. At the 61st American Society of Hematology (ASH) Annual Meeting & Exposition, Geoffrey Uy presented the results of an ongoing phase I/II study (NCT02152956) of flotetuzumab in patients with relapsed/refractory (R/R) AML. The results of this ongoing study, with a special focus on the PIF/ER AML subset, were recently published in Blood and are summarized below.1
Study design
Patients eligible for this phase I/II open-label, single-arm, multi-center, dose escalation study had a diagnosis of non-promyelocytic, R/R AML and met one of the following criteria:
- PIF: Refractory to ≥ 2 induction therapies
- ER: First relapse with initial complete remission (CR) duration < 6 months
- First relapse following unsuccessful salvage treatment
- Second relapse or higher
- Prior failure to hypomethylating agents
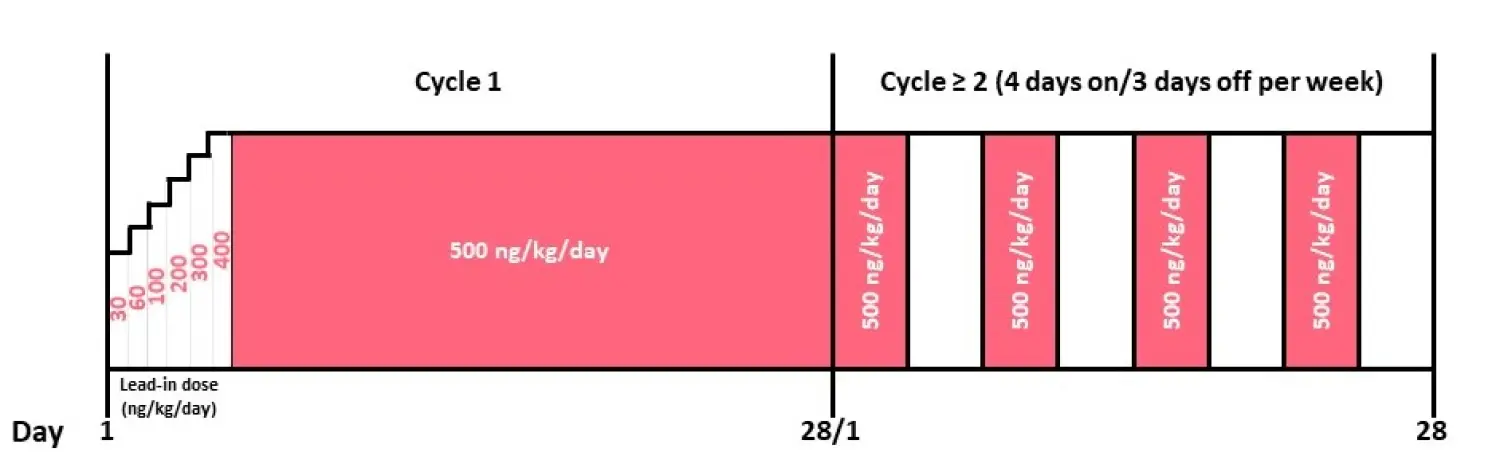
The trial included 88 patients: 42 in the dose escalation phase and 46 who received the recommended phase II dose (RP2D) during the expansion phase. Once the RP2D of 500 ng/kg/day was determined, the expansion dosing schedule (Figure 1), was the following:
- A multi-step lead-in dose (MS-LID) at 30, 60, 100, 200, 300, 400 ng/kg/day for 24 hours each via continuous intravenous infusion (CIV) during Week 1 of Cycle 1 until Day 7
- Dose increase to 500 ng/kg/day CIV on Days 7–28 during Cycle 1
- From Cycle ≥ 2 onwards, flotetuzumab was administered intermittently at 500 ng/kg/day, 4 days on/3 days off per week in 28-day cycles
The primary objective of the study was to determine the maximum tolerated dose/schedule of flotetuzumab and its dose-limiting toxicities (DLTs). Secondary objectives included the assessment of flotetuzumab pharmacokinetics and pharmacodynamics, as well as its clinical efficacy.
Figure 1. Flotetuzumab treatment schedule1
Patient characteristics
Baseline characteristics of the patients included in the study are reported in Table 1. Of the 42 patients included in the dose escalation part, four were treated at the RP2D, so they were also included in the RP2D-evaluable population. Of the 50 patients in the RP2D population, 30 were in the PIF/ER subgroup:
- PIF, n = 24
- ER, n = 6
Table 1. Baseline patient characteristics
|
AML, acute myeloid leukemia; CR, complete remission; ELN, European LeukemiaNet; ER, early relapse; N/A, not applicable; PIF, primary induction failure; RP2D, recommended phase II dose. |
||||
|
Characteristic |
Dose escalation |
Dose expansion RP2D |
RP2D PIF/ER |
|
|---|---|---|---|---|
|
Age |
Median (range) |
64 (29─84) |
64 (27─82) |
59 (27─74) |
|
Gender |
Female, n (%) |
18 (42.9) |
19 (38.0) |
10 (33.3) |
|
AML status at entry |
Primary refractory (≥ 2 induction attempts), n (%) |
15 (35.7) |
24 (48.0) |
24 (80.0) |
|
Early relapse (CR duration ≤ 6 months), n (%) |
8 (19.0) |
6 (12.0) |
6 (20.0) |
|
|
AML risk stratification |
Adverse, n (%) |
13 (31.0) |
26 (52.0) |
18 (60.0) |
|
Intermediate, n (%) |
8 (19.0) |
12 (24.0) |
7 (23.3) |
|
|
Favorable, n (%) |
10 (23.8) |
6 (12.0) |
5 (16.7) |
|
|
Secondary AML |
n (%) |
10 (23.8) |
16 (32.0) |
12 (40) |
|
Number of prior lines of therapy |
Median (range) |
2 (0─9) |
3 (1─9) |
4 (1─9) |
|
Failed induction therapy |
Cytarabine-based induction, n (%) |
N/A |
N/A |
21 (70) |
|
Alternative induction therapy, n (%) |
N/A |
N/A |
3 (10) |
|
|
ER |
n (%) |
4 (9.5) |
6 (12) |
6 (20) |
|
Median duration of CR, months (range) |
N/A |
1.6 (0.8─5.1) |
1.6 (0.8─5.1) |
|
Results
The pharmacokinetic profile of flotetuzumab can be described by the two-compartment model and is linear. The pharmacokinetics and dose-response analysis, performed in all patients who received flotetuzumab with at least one quantifiable concentration value, indicated that the optimal exposure was at the dose of 500 ng/kg/day. At the highest dose tested (700 ng/kg/day), the authors observed a lower exposure because of dose reductions or interruptions due to adverse events.
Safety
The safety of flotetuzumab was assessed in all patients who received at least one dose of flotetuzumab (n = 88). The most common treatment-emergent adverse events (TEAEs) were infusion-related reactions (IRRs) and cytokine release syndrome (CRS). The TEAEs occurring in ˃ 10% of the total population are shown in Table 2.
Table 2. Most common TEAEs (˃ 10%)1
|
CRS, cytokine release syndrome; ER, early relapse; IRR, infusion-related reaction; PIF, primary induction failure; RP2D, recommended phase II dose; TEAE, treatment-emergent adverse event. |
||||||
|
TEAEs |
Dose escalation |
Dose expansion RP2D |
RP2D PIF/ER |
|||
|---|---|---|---|---|---|---|
|
All |
Grade ≥ 3 |
All |
Grade ≥ 3 |
All |
Grade ≥ 3 |
|
|
IRR/CRS |
34 (81.0) |
3 (7.1) |
48 (96.0) |
4 (8.0) |
30 (100) |
1 (3.3) |
|
Nausea |
11 (26.2) |
─ |
14 (28.0) |
─ |
8 (26.7) |
─ |
|
Fatigue |
8 (19.0) |
─ |
6 (12.0) |
1 (2.0) |
3 (10.0) |
1 (3.3) |
|
Pyrexia |
8 (19.0) |
2 (4.8) |
11 (22.0) |
─ |
6 (20.0) |
─ |
|
Peripheral edema |
6 (14.3) |
─ |
15 (30.0) |
1 (2.0) |
8 (26.7) |
─ |
|
Alanine aminotransferase increased |
5 (11.9) |
1 (2.4) |
7 (14.0) |
2 (4.0) |
3 (10.0) |
1 (3.3) |
|
Arthralgia |
5 (11.9) |
1 (2.4) |
7 (14.0) |
1 (2.0) |
4 (13.3) |
─ |
|
C-reactive protein increased |
─ |
─ |
6 (12.0) |
2 (4.0) |
─ |
─ |
|
Diarrhea |
─ |
─ |
11 (22.0) |
─ |
5 (16.7) |
─ |
|
Hypotension |
─ |
─ |
8 (16.0) |
─ |
4 (13.3) |
─ |
|
Decreased appetite |
─ |
─ |
6 (12.0) |
1 (2.0) |
5 (16.7) |
1 (3.3) |
|
Tachycardia |
─ |
─ |
6 (12.0) |
1 (2.0) |
─ |
─ |
|
Myalgia |
─ |
─ |
8 (16.0) |
2 (4.0) |
4 (13.3) |
─ |
|
Dyspnea |
─ |
─ |
9 (18.0) |
3 (6.0) |
4 (13.3) |
2 (6.7) |
|
Platelet count decreased |
7 (16.7) |
5 (11.9) |
7 (14.0) |
6 (12.0) |
3 (10.0) |
3 (10.0) |
|
Lymphocyte count decreased |
6 (14.3) |
5 (11.9) |
6 (12.0) |
4 (8.0) |
─ |
─ |
|
Neutrophil count decreased Treatment-related Non treatment-related |
1 (2.4) |
1 (2.4) |
2 (4.0) |
2 (4.0) |
2 (6.7) |
2 (6.7) |
|
─ |
─ |
1 (2.0) |
1 (2.0) |
1 (3.3) |
1 (3.3) |
|
|
1 (2.4) |
1 (2.4) |
1 (2.0) |
1 (2.0) |
1 (3.3) |
1 (3.3) |
|
The majority of IRR/CRS events (32%) occurred in the first week of treatment and then decreased each week during CIV at 500 ng/kg/day. Most of the patients with IRR/CRS had moderate or mild symptoms (81%). Strategies to reduce the incidence and severity of these events included MS-LID, dose reductions or interruptions for a period of time, and the use of tocilizumab. The MS-LID led to a decrease in the severity of CRS and to an improved mean flotetuzumab dose intensity, as a result of less treatment interruptions or dose reductions. The use of tocilizumab was associated with a decrease in CRS duration. Mean duration of CRS without tocilizumab (n = 42) versus with tocilizumab (n = 13) was 1.8 versus 1.3 days (p = 0.0202).
During the dose escalation part, three patients out of the eight who received flotetuzumab at a dose of 700 ng/kg/day had DLTs (Grade 3 delirium, acute confusional state, or CRS), while no DLTs were observed at the 500 ng/kg/day dose (n = 13). Thus, the RP2D was defined as 500 ng/kg/day.
Efficacy
Response rates are reported in Table 3. As expected by the previously reported increased probability of response to flotetuzumab in patients with immune-infiltrated TME (observed in the PIF/ER subgroup), a better flotetuzumab activity (≥ 50% bone marrow [BM] blast reduction) was observed in patients with PIF/ER (43%, n = 12 out of28), compared to those with late relapse (14%, n = 1 out of 7).
Table 3. Response rates1
|
AML, acute myeloid leukemia; CR, complete remission; CRh, CR with partial hematopoietic recovery; CRi, CR with incomplete hematopoietic recovery; ER, early relapse; MLFS, morphological leukemia-free state; PIF, primary induction failure; PR, partial remission; R/R, relapsed/refractory. |
||
|
|
R/R AML (n=50) |
PIF/ER AML (n=30) |
|---|---|---|
|
CR, n (%) |
6 (12.0) |
5 (16.7) |
|
CR/CRh, n (%) |
9 (18.0) |
8 (26.7) |
|
CR/CRh/CRi, n (%) |
10 (20.0) |
9 (30.0) |
|
CR/CRh/CRi/MLFS/PR, n (%) |
12 (24.0) |
9 (30.0) |
After a median follow-up of 0.8 months (range, 0─25), in patients receiving RP2D:
- Median time-to-first response was 0.84 months (range, 0.8─2.1)
- Median OS was 3.2 months (95% CI, 2.10─6.47)
- For PIF/ER patients (n = 30):
- 6-month survival rate was 42% (95% CI, 0.237─0.5396)
- 12-month survival rate was 20% (95% CI, 0.025─0.377)
- In those (n = 8) achieving CR or CR with partial hematological recovery (CRh):
- Median OS was 10.2 months
- 6-month survival rate was 75% (95% CI, 0.450─1)
- 12-month survival rate was 50% (95%CI, 0.154─0.846)
Better response rates were correlated with higher levels of immune infiltration. CR, CRh, or CR with incomplete hematological recovery (CRi) was achieved by 21% of patients with low immune infiltration, 44.4% of those with intermediate immune infiltration, and by 60% of those with high immune infiltration.
The responses were not correlated with the molecular profile of the treated patients but a baseline increase in inflammatory chemokine score and tumor inflammation signature score were observed in BM samples of patients with PIF/ER compared to those with late relapse.
Unsupervised hierarchical clustering of immune gene expression (770 genes) in baseline BM samples from 38 treated patients showed CR, CRh, or CRi rates of:
- 26.1% with low immune infiltration
- 33.3% with intermediate immune infiltration
- 66.6% with high immune infiltration
The top ten genes associated with CR, CRh, or CRi to flotetuzumab were identified, and their expression was higher in patients with high levels of BM immune infiltration. This ten-gene signature, alone or in combination with the European LeukemiaNet (ELN) risk classifier, was able to predict the response to flotetuzumab better than the ELN risk category alone (AUROC = 0.854 for the ten-gene signature versus 0.672 for the ELN risk classifier; when considered together, AUROC = 0.904).
Conclusion
Flotetuzumab is a promising treatment option for patients with PIF/ER AML who have poor prognosis and limited treatment options. Its clinical activity in this patient population is consistent with recent findings that an immune-infiltrated TME identifies patients more responsive to flotetuzumab. In addition, the identified ten-gene immune signature, alone or in combination with the ELN risk classifier, seemed to be a better predictor of flotetuzumab response than the ELN risk classifier alone. The most frequent adverse events observed were IRR/CRS, but all were manageable.
The trial is ongoing and focused on patients with PIF/ER AML.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the typical turnaround time for next-generation sequencing (NGS) results for AML at your center?