All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View AML content recommended for you
Molecular landscape and prognostic impact of FLT3-ITD insertion site in AML: An analysis of the RATIFY study
During an oral abstract session at the Virtual Edition of the 25th European Hematology Association (EHA) Annual Congress, Frank G. Rücker presented on the molecular landscape and prognostic impact of the FLT3-internal tandem duplication (ITD) insertion site in acute myeloid leukemia (AML),1 from an exploratory analysis of the phase III RATIFY trial (NCT00651261).
FLT3-ITD mutations are present in approximately 25% of adult patients with newly diagnosed AML and are associated with a worse prognosis, especially for patients with a high mutant to wild-type allelic ratio or those with insertions in the β1-sheet of tyrosine kinase domain 1 (TKD1). Other studies have previously shown that FLT3-ITDs in the non-juxtamembrane domain (JMD) confer resistance to a number of FLT3 inhibitors, including midostaurin, a multi-targeted protein kinase inhibitor.1
The AML Hub has previously reported on the results of the RATIFY study, which led to the approval of midostaurin for patients with FLT3-mutated AML by the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) in 2017. Briefly, the results of this study show a significant improvement in the 4-year overall survival (OS) with midostaurin plus intensive chemotherapy compared with intensive chemotherapy alone (51% vs 44%, respectively). The aims of this analysis were to assess the number and structure of FLT3-ITDs in patients enrolled in the study and evaluate the prognostic impact of these insertion sites for the response to midostaurin treatment.
Methods
- Biosamples were available and analyzed by next-generation sequencing (NGS) for 452/555 (81%) of FLT3-ITD positive patients
- The NGS platform used was able to identify mutations present in < 5% of cells
- The insertion site was characterized as JMD only, TKD1 only, or both (JMD/TKD1) for corrective and outcome analysis
Results
- NGS results (Table 1) revealed 908 high-confidence FLT3-ITDs with a median allelic ratio per patient of 0.27
Table 1. Next-generation sequencing results1
|
bp, base pair; cAR, calculated allelic ratio; ITD, internal tandem duplication; NGS, next-generation sequencing; VAF, variant allele frequency |
|
|
NGS result |
Median (range) |
|---|---|
|
Coverage |
3,119 (482–11,616) |
|
Counts |
96 (2–5,234) |
|
VAF, % |
3.32 (0.03–89.49) |
|
Length, bp |
45 (6–246) |
|
cAR/ITD |
0.04 (0.0003–8.51) |
|
cAR/patient |
0.27 (0.0006–10.75) |
- The distribution of the 908 FLT3-ITDs can be seen in Figure 1
- Most patients (46%) exhibited one ITD, with up to nine ITDs seen in a single patient (Figure 1A)
- 70.8% of ITDs were in JMD, whereas 29.2% were in TKD1 (Figure 1B)
Figure 1. Distribution of FLT3-ITD duplications1
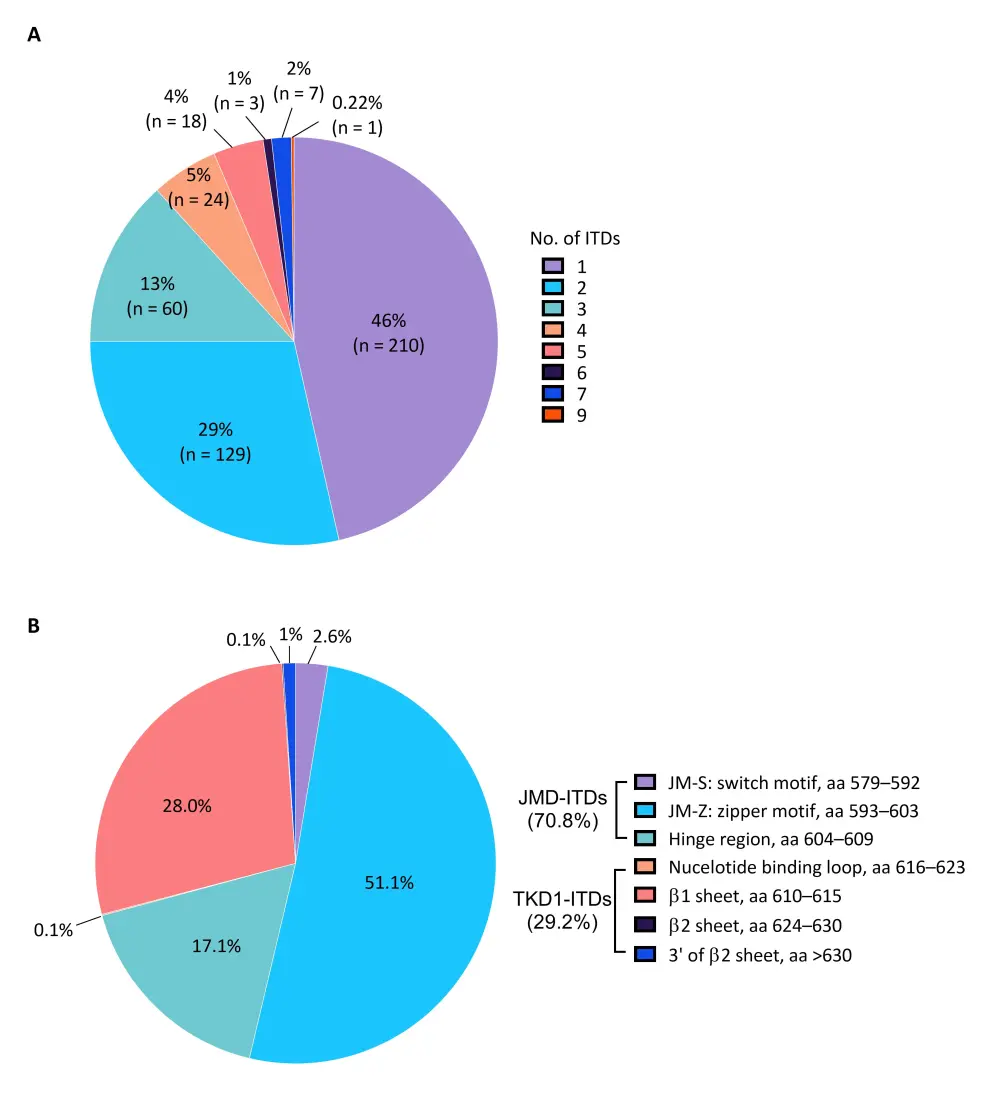
A The number of ITDs per patient. B The location of the ITDs.
aa, amino acid; FLT3, Fms-like tyrosine kinase 3; ITD, internal tandem duplication; JM, juxtamembrane; JMD, juxtamembrane domain; TKD1, tyrosine kinase domain 1
- ITD length was strongly correlated with insertion site (p < 0.001); the more c-terminal the insertion, the longer the inserted fraction
- Insertions in JMD were associated with high NGS-based mutant to wild-type allelic ratio (p < 0.001)
- In 242 patients with multiple ITD integration, the most commonly co-occurring interactions were
- JMD/JMD (37.0%)
- JMD/β1 sheet (20.2%)
- β1 sheet/ β1 sheet (12.2%)
- JMD/hinge region (11.5%)
- In 242 patients with multiple ITD integration, the most commonly co-occurring interactions were
- Clinical characteristics and NPM1 mutation status were compared among the insertion site groups (Table 2)
- The only significant association was the increased prevalence of the NPM1 mutation in the JMD-only insertion site group (p = 0.029)
Table 2. Correlation of FLT3-ITD insertion site with clinical characteristics and NPM1 mutation status1
|
BM, bone marrow; JMD, juxtamembrane domain; NPM1, nucleophosmin 1; TKD1, tyrosine kinase domain 1; WBC, white blood cells |
||||
|
Characteristic |
JMD only (n = 251) |
TKD1 only (n = 117) |
JMD and TKD1 (n = 84) |
p value |
|---|---|---|---|---|
|
Median age, years |
48.3 |
46.3 |
48.1 |
0.171 |
|
Male, % |
40.1 |
54.8 |
48.7 |
0.067 |
|
Median WBC, × 109/L (range) |
40.1 (0.8–329.8) |
53.9 (1.2–144.8) |
39.9 (0.9–205.4) |
0.254 |
|
Median BM blasts, % |
79.5 |
80.0 |
76.0 |
0.489 |
|
NPM1 mutation status, % |
63.1 |
47.9 |
50.0 |
0.029 |
- Complete response was achieved in 274/452 patients (60.6%), and multivariate analysis revealed that two variables were associated with complete response (CR) to induction chemotherapy:
- The number of ITDs were correlated with a lower CR rate (odds ratio, 0.82; 95% CI, 0.70–0.97; p = 0.017)
- NPM1 mutations were correlated with achievement of CR (odds ratio, 1.98; 95% CI, 1.28–3.07; p = 0.002)
- Insertion site had no significant impact on CR
Impact of insertion site on outcome:
- ITD insertion site affected OS (p = 0.032) and the incidence of relapse (p = 0.083)
- Patients with ITDs in the TKD1 site only had the worst OS and the highest incidence of relapse
- OS curves showed a beneficial effect for midostaurin vs placebo across all 3 insertion site subgroups, however the effect on OS was significant for the JMD-only insertion site subgroup only (p = 0.047)
- The multivariate analysis for outcome can be seen in Table 3
- Sole ITD insertion in TKD1 and older age were unfavorable for OS
- NPM1 mutation and hematopoietic stem cell transplantation (HSCT) in first complete remission (CR1) were favorable for OS
- Unfavorable factors for relapse were insertions in TKD1 only, and higher FLT3-ITD calculated allelic ratio
- Sole insertions in JMD, and HSCT in CR1, appeared to decrease relapse risk
Table 3. Multivariable analysis for overall survival and cumulative incidence of relapse1
|
cAR, calculated allelic ratio; CR1, first complete remission; FLT3, Fms like tyrosine kinase 3; HSCT, hematopoietic stem cell transplantation; HR, hazard ratio; ITD, internal tandem duplication; JMD, juxtamembrane domain; NPM1, nucleophosmin 1; TKD1, tyrosine kinase domain 1; WBC, white blood cells |
||||
|
Variable |
Overall survival (n = 358) |
Cumulative incidence of relapse (n = 252) |
||
|---|---|---|---|---|
|
|
HR (95% CI) |
p value |
HR (95% CI) |
p value |
|
TKD1 only (vs JMD only) |
1.61 (1.10–2.35) |
0.014 |
2.20 (1.36–3.56) |
0.001 |
|
TKD1 only (vs JMD/TKD1) |
2.09 (1.24–3.52) |
0.005 |
1.28 (0.78–2.09) |
0.329 |
|
JMD only (vs JMD/TKD1) |
1.30 (0.83–2.05) |
0.254 |
0.58 (0.38–0.88) |
0.010 |
|
Midostaurin treatment |
0.76 (0.57–1.01) |
0.057 |
0.76 (0.53–1.09) |
0.135 |
|
FLT3-ITD cAR (log2) |
1.07 (0.99–1.15) |
0.104 |
1.15 (1.04–1.28) |
0.008 |
|
No. of ITDs |
1.11 (0.80–1.54) |
0.530 |
1.06 (0.90–1.26) |
0.463 |
|
WBC (log2) |
1.03 (0.58–1.81) |
0.930 |
1.06 (0.50–2.22) |
0.879 |
|
Age |
1.02 (1.00–1.03) |
0.033 |
1.00 (0.98–1.02) |
0.976 |
|
NPM1 mutation |
0.57 (0.42–0.78) |
<0.001 |
0.73 (0.50–1.07) |
0.105 |
|
HSCT in CR1 |
0.38 (0.24–0.58) |
<0.001 |
0.47 (0.29–0.74) |
0.001 |
Conclusion
The number and location of ITDs as well as NPM1 mutations were predictive of outcome. NPM1 mutations and HSCT in CR1 were associated with improved outcome. ITDs in TKD1 only were unfavorable for OS and cumulative incidence of relapse. Patients with ITDs in TKD1 only had significantly inferior outcomes compared with those with ITDs in JMD-only or both domains. Patients with ITDs in JMD only benefited significantly from midostaurin treatment, whereas no benefit was seen in those with ITDs in TKD1 only, which confirms findings from earlier preclinical studies. However, it is important to note that there was a smaller number of patients in the TKD1-only group.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?