All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Impact of RUNX1, RAS, and del(7)/del(7q) genetic abnormalities on prognosis and response to venetoclax
Mutational profiling is becoming increasingly important in the diagnosis and treatment of patients with acute myeloid leukemia (AML), particularly to identify genes that may impact prognosis and treatment responses. Here, we look at a few genetic abnormalities, RUNX1 gene mutations, RAS gene mutations, del(7), and del(7q), in terms of their clinical significance in AML.
Mutations in RUNX1 occur in up to 10% of patients with newly diagnosed (ND) AML and are generally associated with an adverse prognosis in the absence of any favorable risk markers.1 Mutations in RAS are seen in 10–25% of patients with AML, but currently have unknown prognostic significance. However, RAS mutations have been identified as a potential resistance mechanism to treatment with FLT3, IDH, and BCL2 inhibitors.2 The cytogenetic events del(7) and del(7q) appear in 20–30% of patients with ND AML and generally confer an adverse prognosis.3 The presence of these abnormalities may affect response to therapeutics, such as venetoclax, a BCL2 inhibitor that is efficacious in combination with hypomethylating agents (HMAs), or low-dose cytarabine, particularly in older patients with AML who are unfit for chemotherapy.1,3
Below, we summarize three recent articles published by Venugopal et al.1, Rivera et al.2, and Abbas et al.3, which evaluated the prognostic significance of these genetic abnormalities and assessed their impact on response to treatment with and without venetoclax.
The impact of RUNX1 mutations1
Study design and patient characteristics
This was a retrospective cohort study of 907 adults with ND AML who received frontline therapy of intensive chemotherapy (intermediate- or high-dose cytarabine-based combinations) or low-intensity therapy (low-dose cytarabine or a HMA) with or without venetoclax between 2009 and 2020. Conventional G-band karyotyping was performed on bone marrow samples at diagnosis, alongside next-generation sequencing (NGS).
SRSF2 was most commonly co-mutated with RUNX1
Overall, 15% of patients harbored RUNX1 mutations (RUNX1mut).
- These patients were significantly older and less likely to have an adverse karyotype, while more likely to have secondary AML than patients with wild-type RUNX1 (RUNX1wt).
- 26% received intensive chemotherapy, 48% received low-intensity therapy without venetoclax, and 26% received low-intensity therapy with venetoclax.
- 20% had ≥2 RUNX1 mutations and 33% had variable allele frequency (range, 1–96%).
- SRSF2, ASXL1, IDH1, or IDH2 were commonly co-mutated with RUNX1 and TP53 was less likely to be co-mutated (Figure 1).
Figure 1. Mutations detected alongside RUNX1mut and RUNX1wt*
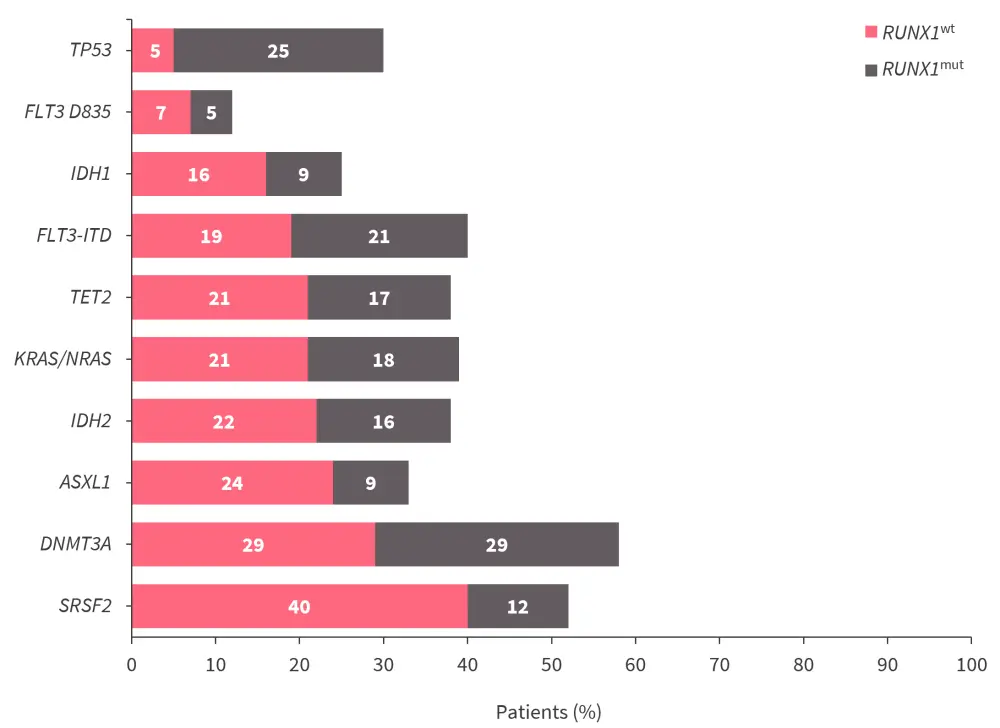
RUNX1mut, mutated RUNX1; RUNX1wt, wild-type RUNX1.
*Data from Venugopal, et al.1
Response rates were similar across mutational subtype and treatment groups
The overall complete remission (CR) rate was 54%, with a composite CR (CCR; CR + CR with incomplete hematological recovery) rate of 64%. There were no significant differences in CCR rates in patients with RUNX1mut and RUNX1wt across the intensive chemotherapy, low-intensity therapy, and low-intensity therapy plus venetoclax treatment groups.
Survival outcomes
The median follow-up of the whole cohort was 41.7 months. The median time to relapse was 29.8 months, relapse-free survival (RFS) was 13.2 months, and overall survival (OS) was 14.5 months.
- In patients treated with intensive chemotherapy or low-intensity therapy without venetoclax, 2-year OS rates were similar regardless of RUNX1 mutational status.
- In patients with RUNX1mut treated with low-intensity therapy plus venetoclax, there was a trend towards improved OS compared with patients with RUNX1wt (Table 1).
- Among patients with RUNX1mut, 2-year OS rates were similar between those treated with intensive chemotherapy and low-intensity chemotherapy plus venetoclax (p = 0.47) despite patients in the low-intensity therapy plus venetoclax group being generally older and less fit.
Table 1. Survival outcomes by treatment group and RUNX1 mutational status*
|
IC, intensive chemotherapy; LIT, low-intensity therapy; OS, overall survival; Ven, venetoclax; RUNX1mut, mutated RUNX1; RUNX1wt, wild-type RUNX1. |
||||||
|
Outcome
|
IC |
LIT without Ven |
LIT with Ven |
|||
|---|---|---|---|---|---|---|
|
RUNX1mut |
RUNX1wt |
RUNX1mut |
RUNX1wt |
RUNX1mut |
RUNX1wt |
|
|
Median OS, months |
20.2 |
43.6 |
14.9 |
9.0 |
25.1 |
11.3 |
|
1-year OS, % |
78 |
70 |
56 |
43 |
63 |
47 |
|
2-year OS, % |
50 |
56 |
20 |
23 |
54 |
33 |
|
p value |
0.72 |
0.83 |
0.12 |
|||
The impact of RAS mutations2
Study design and patient characteristics
This was a retrospective cohort study of 1,410 patients with ND AML treated between 2011 and 2020 with intensive chemotherapy with or without venetoclax, the HMAs decitabine or azacitidine with or without venetoclax, or cladribine plus low-dose cytarabine with or without venetoclax. Karyotypic analysis was performed on ≥20 metaphase cells and NGS was used for mutational analysis.
Mutated RAS was harbored by 20% of patients. Compared with patients with RASwt, patients with RASmut:
- had a higher median white blood cell (WBC) count and lower median platelet count;
- were more likely to have a treated secondary AML (defined as having a previous diagnosis of myelodysplastic syndromes or myeloproliferative neoplasms and having received ≥1 treatment prior to AML transformation);
- were more likely to have a favorable or non-diploid intermediate karyotype; and
- were less likely to have an adverse karyotype.
FLT3 was most commonly co-mutated with RAS
As shown in Figure 2, patients with RASmut:
- were more likely to have co-mutated UA2F1 (p = 0.01), PTPN11 (p = 0.002), BCOR (p = 0.01), EZH2 (p = 0.02), or BCORL1 (p = 0.04); and
- were less likely to have co-mutated TP53 (p < 0.001).
Figure 2. Percentage of co-mutations by RAS mutation status*
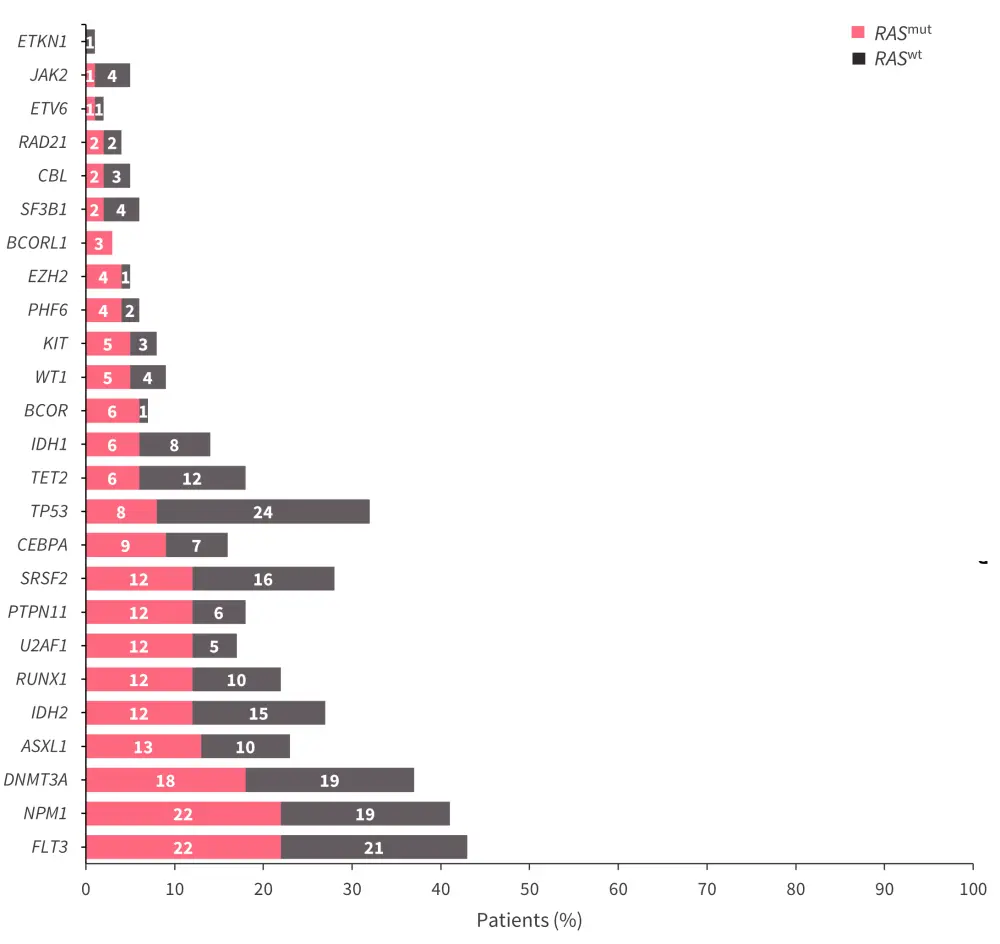
RASmut, mutated RAS; RASwt, wild-type RAS.
*Adapted from Rivera, et al.2
Mutations in RAS were associated with lower remission rates following treatment with HMA plus venetoclax
- No significant differences in CCR rate were observed between mutational groups in patients who received high-dose cytarabine or cladribine plus low-dose cytarabine, with or without venetoclax, or HMA monotherapy (Figure 3).
- In patients who received HMA plus venetoclax, patients with RASmut had a significantly lower CCR rate than patients with RASwt (p = 0.006; Figure 3).
Figure 3. CCR rates by treatment and RAS mutational status*
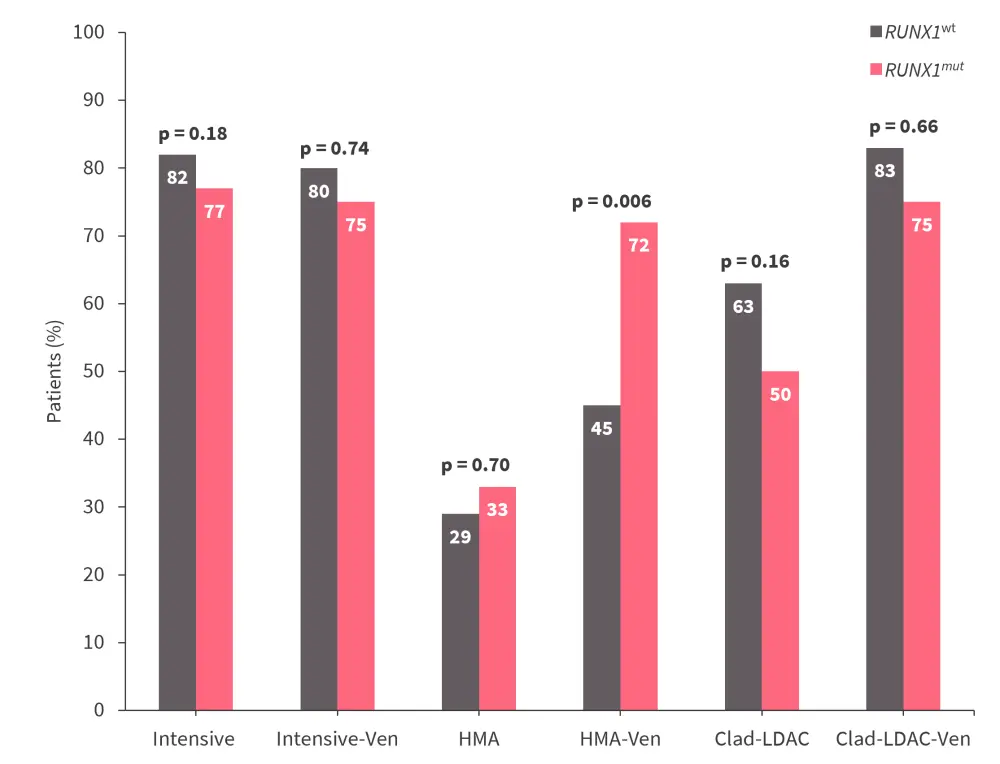
Clad-LDAC, cladribine plus low-dose cytarabine; CCR, composite complete remission; HMA, hypomethylating agent; RASmut, mutated RAS; RASwt, wild-type RAS; Ven, venetoclax.
*Adapted from Rivera, et al.2
Survival outcomes
The median follow-up within the study population was 43 months. Patients with RASmut had an improved 3-year survival rate of 38%, compared with 28% in patients with RASwt (p = 0.01).
- In the intensive chemotherapy treatment group, patients with RASmut had a survival benefit compared to RASwt (median, 85 months vs 29 months; p = 0.04).
- There was no significant difference in OS between patients with RASmut and RASwt in the HMA (median, 5 months vs 7 months; p = 0.89) and cladribine plus low-dose cytarabine (median, 11 months vs 11 months; p = 0.39) treatment groups.
- The addition of venetoclax was associated with a trend for better OS in the cladribine plus low-dose cytarabine treatment groups, but not in the HMA treatment group.
- The multivariable analysis model found:
- intensive chemotherapy gave a 60% reduction in the risk of death (hazard ratio, 0.42; 95% confidence interval, 0.2–0.6; p < 0.001).
- The addition of venetoclax did not significantly reduce the risk of death (hazard ratio, 0.68; 95% confidence interval, 0.4–1.1; p = 0.13).
The impact of del(7) and del(7q) genetic abnormalities.3
Study design and patient characteristics
This was a retrospective cohort study of 243 adult patients with ND AML with either del(7) or del(7q) treated between 2010 and 2020 with high-intensity treatment (including standard or high-dose cytarabine-based therapies with or without venetoclax) or low-intensity treatment (including HMAs, low-dose cytarabine, or nucleoside analog-based therapy, such as cladribine or clofarabine, with or without venetoclax).
Cytogenetic analysis was performed by G-banding technique on ≥20 metaphase cells. Patients with monosomy 7 or del(7q) were analyzed using amplicon-based targeted NGS. Alterations to the TP53 gene were defined by either TP53 gene mutations, loss in chromosome 17, or segmental loss in chromosome 17p.
Overall, 69% of patients had del(7) and 31% of patients had a del(7q) abnormality. Patient characteristics were similar between the cytogenetic subgroups.
TP53 was the most commonly occurring mutation
- TP53mut co-occurred with del(7) or del(7q) in 97 of 178 (54%) patients tested, of which 33% also had deletions in chromosome 17 or 17p.
- Deletions in chromosome 17 or 17p were harbored by 33% of patients with TP53mut and 86% of patients with TP53wt.
- The frequency of TP53mut was similar between patients with del(7) and del(7q) (p = 0.9).
- Alterations to TP53 were significantly associated with complex cytogenetics (p < 0.0001).
The most common co-occurring cytogenetic abnormality was chromosome 5q deletions, at a similar rate between patients with del(7) and del(7q) (37.5% vs 42.7%; p = 0.4). Patients with del(7) and del(7q) had very similar molecular and co-occurring cytogenetic profiles.
TP53 mutations conferred poorer outcomes
There was a 48.5% CCR rate similarity between patients with del(7) (49.4%) and del(7q) (46.6%). In patients with TP53mut versus TP53wt, the CCR rate was:
- 42.2% vs 64.2% in patients with del(7), respectively; and
- 44.7% vs 52.4% in patients with del(7q), respectively.
The median OS was 7.3 months (range, 0.1–115.8 months).
- Del(7) and del(7q) subgroups were similar in regard to OS (p = 0.2) and remission duration (p = 0.16).
- RFS was significantly longer in patients with del(7q) compared with del(7) (p = 0.049).
- Patients with del(7) or del(7q) who had TP53 alterations had significantly worse OS (p < 0.0001) and remission duration (p = 0.0035) but not RFS (p = 0.16) compared with patients with TP53wt (Figure 4).
Figure 4. Survival outcomes stratified by TP53 mutational status*
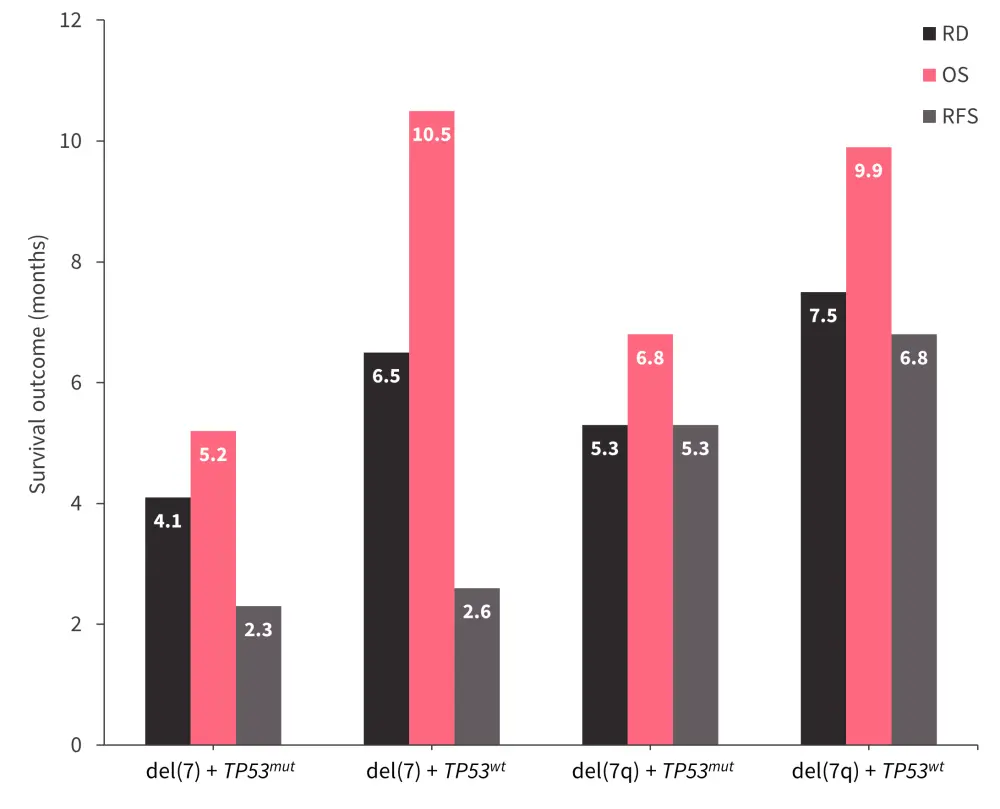
OS, overall survival; RD, remission duration, RFS, relapse-free survival; TP53mut, mutated TP53; TP53wt, TP53 wild-type.
*Data from Abbas, et al.3
Clinical outcomes were not improved with venetoclax-based therapies
In total, 16% of patients received venetoclax as part of their frontline therapy. In patients treated with versus without venetoclax, the CCR rate was:
- 54.8% vs 48.2% in those with del(7), respectively; and
- 75.0% vs 43.3% in those with del(7q), respectively
In patients with del(7), venetoclax-based therapies were associated with worse survival outcomes. Compared with all other treatment groups, those with del(7) who received venetoclax showed:
- shorter median OS, 5.8 months (log-rank p = 0.47);
- poorer median RFS, 0.1 months (log-rank p < 0.0001); and
- shorter median duration of remission, 2.2 months (log-rank p = 0.0015).
In addition, no improvement in OS, RFS, or remission duration was seen with venetoclax in patients with del(7q). Within TP53-defined subgroups, survival was not improved with venetoclax in patients with TP53mut or TP53wt and OS was notably reduced in patients with del(7) and TP53wt (p = 0.0017).
Conclusion
All three studies highlight the role mutational profiling can play in predicting the prognosis of patients with AML and how genetic abnormalities may affect the response to treatment. In some cases, the prognosis associated with the presence of certain mutations could be exacerbated by particular treatments, for example venetoclax-based therapies. These studies highlight the need for further investigation into the association between mutational profiles, including the presence of co‑mutations, and the type of treatment received, alongside the impact on risk stratification.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?