All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Evaluating predictive factors for post-HSCT survival in secondary AML
Patients with secondary acute myeloid leukemia (sAML) have poor clinical outcomes, even after intensive chemotherapy, and allogeneic hematopoietic stem cell transplantation (HSCT) remains the only curative treatment option for these high-risk patients. It is unclear whether disease burden prior to HSCT holds similar prognostic value for sAML as for de novo AML, and the influence of cytogenetic and molecular risk at diagnosis on outcomes for patients with sAML, compared with de novo patients, is also unknown.
Data evaluating the impact of pre-HSCT disease burden and European LeukemiaNet (ELN) risk classification at diagnosis on survival for patients with sAML and de novo AML were presented by Claudia Nuñez-Tórrez in two abstracts during the 47th Annual Meeting of the European Society for Blood and Marrow Transplantation (EBMT).1,2 Here, we summarize their findings.
Prognostic impact of pre-HSCT disease burden
A retrospective analysis was performed on 108 patients with de novo AML (n = 49) or sAML (n = 59) to assess:
- post-HSCT event-free survival (EFS) and overall survival (OS) for sAML compared with de novo AML;
- the impact of achieving a complete remission (CR) before HSCT on EFS and OS; and
- the impact of achieving CR and measurable residual disease (MRD) by flow cytometry on EFS and OS.
Just over half of patients with de novo AML had recurrent cytogenetic abnormalities. Most sAML cases (63%) were classified as AML with myelodysplasia-related changes; Ph-negative blast phase myeloproliferative neoplasms and therapy-related AML accounted for 29% and 8% of cases, respectively.
Selected patient, disease, and treatment characteristics are shown in Table 1. Of note, patients with sAML were older, more frequently had an adverse cytogenetic risk profile, and were more likely to be chemorefractory, than patients with de novo AML.
Table 1. Selected patient, disease, and treatment characteristics*
|
AML, acute myeloid leukemia; CR, complete remission; ELN, European LeukemiaNet; HSCT, hematopoietic stem cell transplant; sAML, secondary AML. |
||
|
Characteristic |
De novo AML |
sAML |
|---|---|---|
|
Median age at HSCT, years (range) |
49 (21–68) |
57 (20–69) |
|
ELN classification, % |
|
|
|
CR after induction, % |
89.4 |
71.2 |
|
Disease state prior to HSCT, % |
|
|
|
Conditioning intensity, % |
|
|
|
Donor type, % |
|
|
At a median follow-up of 12 months, EFS and OS after HSCT were significantly inferior for patients with sAML compared with patients with de novo AML; the median EFS was 7 months vs not reached (hazard ratio [HR], 2.6; p < 0.001) and the median OS was 10 months vs not reached (HR, 3; p < 0.001).
- When assessing the impact of pre-HSCT disease state, patients with active disease had worse EFS and OS than those with a CR (EFS: HR, 3.5; p < 0.001; OS: HR, 3.2; p < 0.001).
- In a subanalysis according to AML type, patients with de novo AML who achieved a CR before transplant had an improved EFS and OS compared with those transplanted with active disease (EFS: HR, 6.2; p < 0.001; OS: HR, 6.5; p < 0.001).
- However, the improvement in EFS was less significant for patients with sAML who achieved CR (HR, 2.5; p = 0.003), and there was no significant difference in OS for patients with sAML in CR compared with those with active disease (HR, 1.9; p = 0.05).
The variables identified as significant predictors of EFS and OS in multivariate analysis were AML type (sAML vs de novo AML) and pre-HSCT disease state (CR vs active disease) (Table 2).
Table 2. Factors associated with EFS and OS in univariate and multivariate analysis*
|
AML, acute myeloid leukemia; CR, complete remission; EFS, event-free survival; HR, hazard ratio; HSCT, hematopoietic stem cell transplant; MAC, myeloablative conditioning; OS, overall survival; RIC, reduced-intensity conditioning; sAML, secondary AML. |
||||
|
Variable |
EFS (HR, p value) |
OS (HR, p value) |
||
|---|---|---|---|---|
|
Univariate |
Multivariate |
Univariate |
Multivariate |
|
|
Age >60 years |
2, 0.01 |
— |
2.5, 0.001 |
— |
|
sAML vs de novo AML |
2.6, 0.001 |
2.1, 0.04 |
3, 0.001 |
2.6, 0.02 |
|
Intermediate/adverse vs favorable risk |
3.6, 0.001 |
— |
3.1, 0.03 |
— |
|
CR vs active disease after induction |
2.2, 0.008 |
— |
— |
— |
|
CR vs active disease pre-HSCT |
3.5, <0.001 |
2.4, 0.02 |
3.2, <0.001 |
2.2, 0.04 |
|
RIC vs MAC |
2, 0.01 |
— |
2.2, 0.006 |
— |
Of 89 patients in CR pre-HSCT, 86 had MRD status determined by flow cytometry; 63 were MRD-negative and 23 were MRD-positive.
- Patients in CR with MRD-negative status trended towards improved 2-year EFS, compared with MRD-positive patients (p = 0.09).
- Prospective studies are required to determine whether MRD status has equivalent prognostic impact in sAML and de novo AML.
Prognostic impact of cytogenetic and molecular risk
The influence of ELN classification at diagnosis on survival outcomes was assessed in a retrospective analysis of a slightly modified patient cohort to the one presented above, with the addition of three patients with de novo AML (N = 111; de novo AML n = 52, sAML n = 59).
Proportional ELN classification at diagnosis for the de novo and sAML patient cohorts is shown in Figure 1.
Figure 1. ELN risk classification at diagnosis*
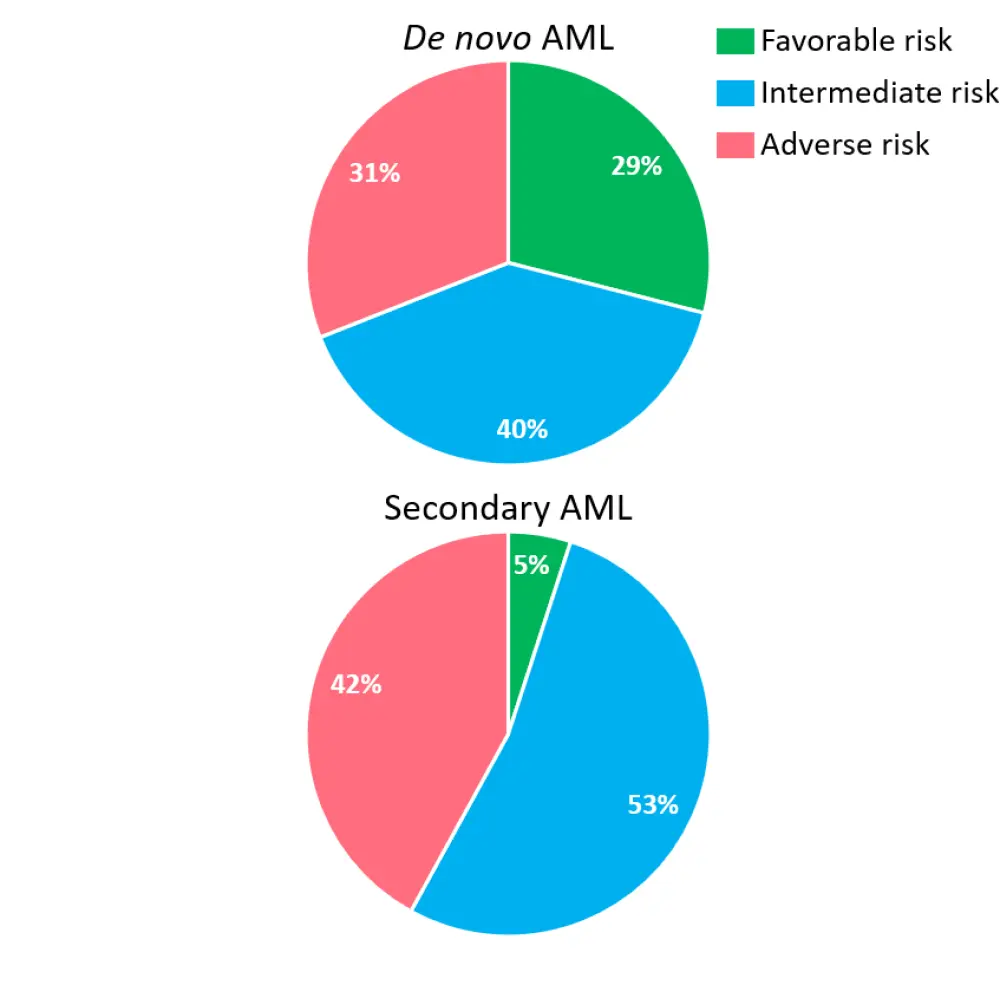
Median EFS and OS for patients with de novo AML and sAML according to ELN risk classification are shown in Table 3. Whilst patients with de novo AML and a favorable risk profile had improved outcomes compared with patients with adverse risk, the ELN risk classification did not influence survival for patients with sAML.
Table 3. EFS and OS according to ELN risk classification*
|
AML, acute myeloid leukemia; CI, confidence interval; EFS, event-free survival; ELN, European LeukemiaNet; HR, hazard ratio; NR, not reached; OS, overall survival; sAML, secondary AML. |
||||
|
Outcome by AML type |
ELN risk classification |
HR (95% CI) |
||
|---|---|---|---|---|
|
Favorable |
Intermediate |
Adverse |
||
|
De novo AML |
|
|
|
|
|
sAML |
|
|
|
|
Summary
Patients with sAML are more likely to be chemorefractory and have inferior survival compared with patients with de novo AML. Unlike for patients with de novo AML, the achievement of a CR prior to transplantation was not so strongly predictive of EFS and had no significant association with OS for patients with sAML. Moreover, transplant results for patients with sAML were not influenced by ELN risk classification at diagnosis.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?