All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Effect of gilteritinib treatment response and FLT3 mutation clearance on overall survival in R/R FLT3-mutated AML
The safety and efficacy of gilteritinib in patients with relapsed/refractory (R/R) acute myeloid leukemia (AML) and fms-like tyrosine kinase 3 (FLT3) mutations has previously been demonstrated in the phase I/II CHRYSALIS study. The oral FLT3 inhibitor has since been approved in the U.S. and Europe for R/R FLT3-mutated AML, based on the results from the subsequent phase III ADMIRAL study (NCT02421939).
The persistence of measurable residual disease (MRD), beyond morphologic complete remission (CR), is an established indicator of adverse prognosis in AML. The monitoring of FLT3 mutational burden is likely to be informative for patients with FLT3-mutated AML treated with FLT3 inhibitors, however its value as a clinically meaningful marker of MRD is a subject of debate due to the unstable nature of these mutations.1
In a publication in Cancer Medicine, AML Hub Scientific Advisory Board member, Jessica Altman, and colleagues discuss the impact of gilteritinib treatment response and FLT3-internal tandem duplication (ITD) mutation clearance on the survival of patients with R/R FLT3-ITD-mutated AML in the CHRYSALIS trial.2 Here, we are pleased to report their findings.
Study design
CHRYSALIS (NCT02014558) was a phase I/II open-label, dose-escalation/ expansion study of single-agent gilteritinib in the treatment of patients with R/R AML.
- A total of 108 patients with FLT3-ITD-positive R/R AML from the CHRYSALIS study were evaluated for FLT3-ITD mutation clearance, using a combined polymerase chain reaction/next-generation sequencing approach to assess FLT3-ITD variant allele frequency (VAF) in genomic DNA from bone marrow aspirates. FLT3-ITD mutation clearance was classified as FLT3-ITD VAF ≤ 10–4.
- The impact of treatment response (composite CR [CRc] and CR/CR with partial hematologic recovery [CRh]) with FLT3-ITD mutation clearance on overall survival was assessed in a subset of 95 patients who had received ≥ 80 mg/day gilteritinib.
- Mutation clearance was additionally assessed in a cohort of 56 patients receiving 120 mg/day gilteritinib, which was identified in CHRYSALIS as the recommended dose for subsequent clinical trials.
Key findings
Baseline characteristics were representative of the CHRYSALIS trial population.
- FLT3-ITD mutation clearance was achieved in 10 out of 108 patients (9.3%), all of whom received ≥ 80 mg/day gilteritinib.
- Median baseline FLT3-ITD VAF was similar for patients with and without FLT3-ITD mutation clearance (median VAF 0.4205 and 0.4056, respectively).
- Among the 95 patients (out of a total 108) receiving ≥ 80 mg/day gilteritinib, 10 patients achieved FLT3-ITD mutation clearance (10.5%). Median overall survival (OS) was 76.8 weeks (95% CI, 18.6–NR) for patients with FLT3-ITD mutation clearance, and 30.6 weeks (95% CI, 22.4–37.7) for those without mutation clearance (HR, 0.663; 95% CI, 0.298–1.475).
- FLT3-ITD mutation clearance status according to treatment response for patients receiving ≥ 80 mg/day gilteritinib is shown in Figure 1.
Figure 1. FLT3-ITD mutation clearance status according to treatment response2
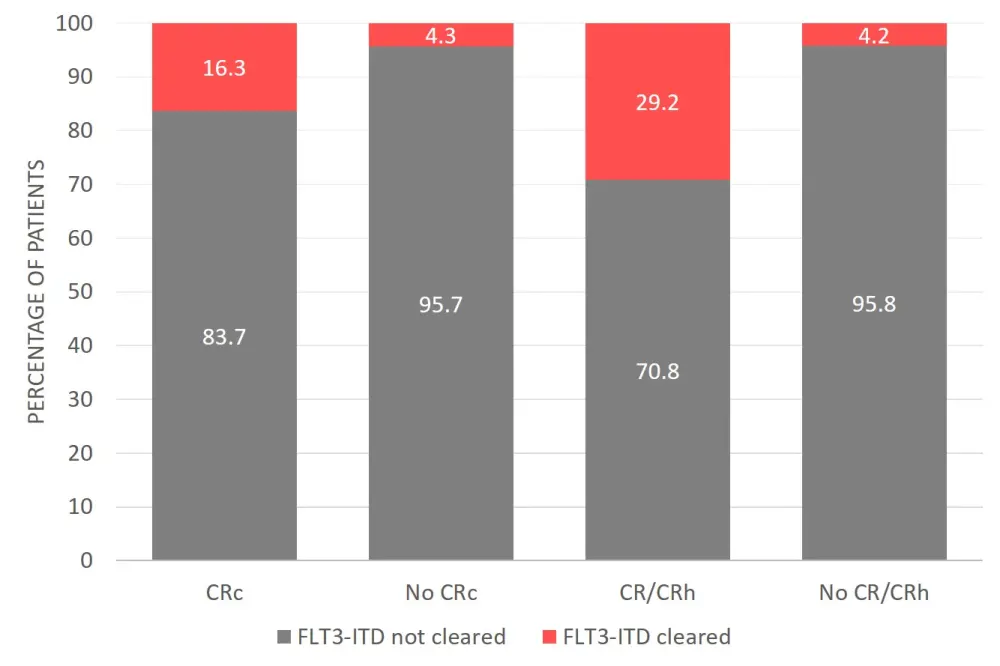
CR, complete remission; CRc, composite CR; CRh, CR with partial hematologic recovery.
- A best overall response of CRc was achieved in 51.6% of patients receiving ≥ 80 mg/day gilteritinib.
- In patients experiencing CRc, there was a trend towards longer OS in the 16.3% with FLT3-ITD mutation clearance (131.4 weeks; 95% CI, 18.6–NR), compared to those without mutation clearance (43.3 weeks; 95% CI, 27.7–56.9; HR, 0.416; p = 0.066).
- Median duration of CRc was 60.0 weeks and 12.1 weeks for patients with and without FLT3-ITD mutation clearance, respectively.
- A best overall response of CR/CRh was achieved in 25.3% of patients receiving ≥ 80 mg/day gilteritinib.
- Median duration of CR/CRh was not reached for patients with FLT3-ITD mutation clearance and was 19.4 weeks for patients without mutation clearance (HR, 0.454; 95% CI, 0.117–1.752).
- Among 34 patients assessed for mutation clearance in the cohort receiving 120 mg/day gilteritinib, six patients had FLT3-ITD mutation clearance and nine achieved CR/CRh.
- Median OS was 70.6 weeks for patients who achieved CR/CRh and 41.7 weeks for those who did not achieve CR/CRh; survival probability at 52 weeks was 66.7% and 20.2%, respectively.
Conclusion
Gilteritinib induced morphologic remission and mutation clearance in patients with R/R FLT3-ITD mutated AML. Of patients receiving ≥ 80 mg/day gilteritinib in the CHRYSALIS trial, over half achieved a CRc and 10% had FLT3-ITD mutation clearance.
Furthermore, patients achieving CRc or CR/CRh were more likely to have FLT3-ITD clearance, and a longer OS, than patients who did not achieve deep remissions, indicating a potential relationship between FLT3-ITD clearance and prognosis.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?