All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Editorial theme | Frequency of oral mucositis in patients with AML post-allogeneic hematopoietic cell transplantation
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a beneficial treatment option for patients with acute myeloid leukemia (AML). Prior to transplantation, patients require myeloablative conditioning (MAC) and although intensive conditioning decreases the risk of relapse, it induces high toxicity. Reduced intensity conditioning (RIC) as an alternative to MAC, helps to reduce toxicity but increases the risk of transplant rejection. Oral mucositis as a result of cytostatic, impaired immune system function and decreased salivation, is one of the most common oral complications of high-dose chemotherapy observed in early hematopoietic stem cell transplantation (HSCT). Oral erosions and ulcers that develop because of oral mucositis, serve as a portal of entry for viral, fungal, and bacterial antigens, and these infections, consequently, increase morbidity and mortality post-HSCT. However, as the use of allo-HSCT increases gradually in older adults and patients with comorbidities, there is a need to understand the occurrence of oral mucositis in patients with AML after allo-HSCT.
Wysocka-Słowik et al,1 recently published a study in Annals of Hematology, investigating the frequency and severity of oral mucositis depending on the type of conditioning regimen in patients with AML post-allo-HSCT.
Study design
A prospective cohort study in patients diagnosed with AML who had undergone allo-HSCT. Eligible patients (N = 80) were allocated to either MAC (n = 54) or RIC (n = 26) regimen based on age and comorbidities. Cytostatics included in the MAC group were fludarabine, busulfan, melphalan, and treosulfan, individually adjusted to each patient’s profile and applied in appropriate proportions as FluBu4, and the RIC group included fludarabine, busulfan, cytarabine, and total body irradiation (TBI), used as FluBu2 or Flu-CyTBI.
- Patients were examined at three time points: preliminary examination (from Day −10 to −7); first examination (from Day +3 to +7); and secondary examination (from Day +8 to +14).
- The primary endpoint was intensity of oral mucositis evaluated according to the five-point scale recommended by World Health Organization (WHO) (Table 1).
Table 1. Five-point scale*
|
WHO, World Health Organization. |
|
|
Mucositis grade† |
WHO criteria |
|---|---|
|
0 |
No signs |
|
1 |
Oral soreness +/− erythema, no erosions, oral discomfort |
|
2 |
Oral erythema, ulcers; solid diet tolerated |
|
3 |
Diffuse oral erythema, ulcers; liquid diet only |
|
4 |
Severe inflammation, diffuse inflammatory-necrotic lesions; alimentation not possible |
- Prevention of oral mucositis in both groups involved maintenance of good oral hygiene. All patients were recommended supersaturated calcium phosphate, electrolyte mouth rinse, and fluconazole. For oral mucositis, multipurpose mouthwash, and antifungals (benzocaine/natrium, boricum/glicerini, thymol/glycerini, and colistin/gentamycin/nystatin, amphotericin B) were advised along with morphine and tramadol for pain management.
Baseline characteristics
Patients in the MAC group comprised 30 women and 24 men, with a mean age of 42±12 years, and 12 women and 14 men with a mean age of 56±13 years in the RIC group.
Results
All patients
At preliminary examination, 84% of all patients demonstrated Grade 0 mucositis. However, at the first posttransplant examination this decreased to 34% of patients demonstrating Grade 0 mucositis, and a further decrease to 26% after the second posttransplant examination (Table 2), representing a statistically significant difference between first and second examination (p < 0.0001).
Table 2. Incidence of oral mucositis*
|
WHO, World Health Organization. |
|||
|
Mucositis grade† |
All patients (N = 80) |
||
|---|---|---|---|
|
Preliminary examination |
First examination |
Second examination |
|
|
0 |
84 |
34 |
26 |
|
1 |
13 |
43 |
33 |
|
2 |
4 |
15 |
28 |
|
3 |
0 |
6 |
10 |
|
4 |
0 |
2 |
4 |
- Grade 1 mucositis was observed in 13% of the entire cohort at preliminary examination, 43% at first, and 33% at second examination. Differences between preliminary and first, and second examinations were statistically significant (p < 0.0001 and p = 0.0020, respectively).
- Patients with Grade 2 mucositis in the entire cohort were lower at preliminary examination compared to first and second examinations (p = 0.0121 and p < 0.0001, respectively).
- The difference between the incidence of Grade 3 mucositis in all patients between preliminary and first, and second examination was statistically significant (p = 0.0261 and p = 0.0037, respectively).
- No statistically significant differences were observed in the incidence of Grade 4 mucositis in the entire cohort.
MAC and RIC
- No statistically significant difference was observed at preliminary examination between MAC and RIC groups (as shown in Table 3).
Table 3. Incidence of oral mucositis based on type of conditioning*
|
examin., examination; MAC, myeloablative conditioning; RIC, reduced intensity conditioning; WHO, World Health Organization. |
||||||
|
Mucositis grade† |
MAC (n = 54) |
RIC (n = 26) |
||||
|---|---|---|---|---|---|---|
|
Preliminary examin. |
First examin. |
Second examin. |
Preliminary examin. |
First examin. |
Second examin. |
|
|
0 |
85 |
26 |
17 |
84 |
50 |
46 |
|
1 |
13 |
46 |
31 |
12 |
35 |
35 |
|
2 |
2 |
19 |
33 |
4 |
8 |
15 |
|
3 |
0 |
7 |
15 |
0 |
4 |
0 |
|
4 |
0 |
2 |
4 |
0 |
4 |
4 |
- Patients in the MAC group compared with the RIC group, demonstrated a significantly higher incidence of mucositis (74% vs 50% at first examination, and 83% vs 53% at second examination, respectively) (Figure 1).
- At the first examination, 26% and 50% patients in the MAC and RIC group, respectively, demonstrated Grade 0 mucositis and the difference between the two groups was statistically significant (p = 0.0335). The incidence of Grade 0 mucositis decreased further at second examination, with 17% and 47% in the MAC and RIC group, respectively (p = 0.0059) (Figure 1).
- The differences in the incidence of oral mucositis between the preliminary and posttransplant examinations were statistically significant (p < 0.0001 and p = 0.0020, respectively) in both MAC and RIC groups.
Figure 1. Incidence of oral mucositis*
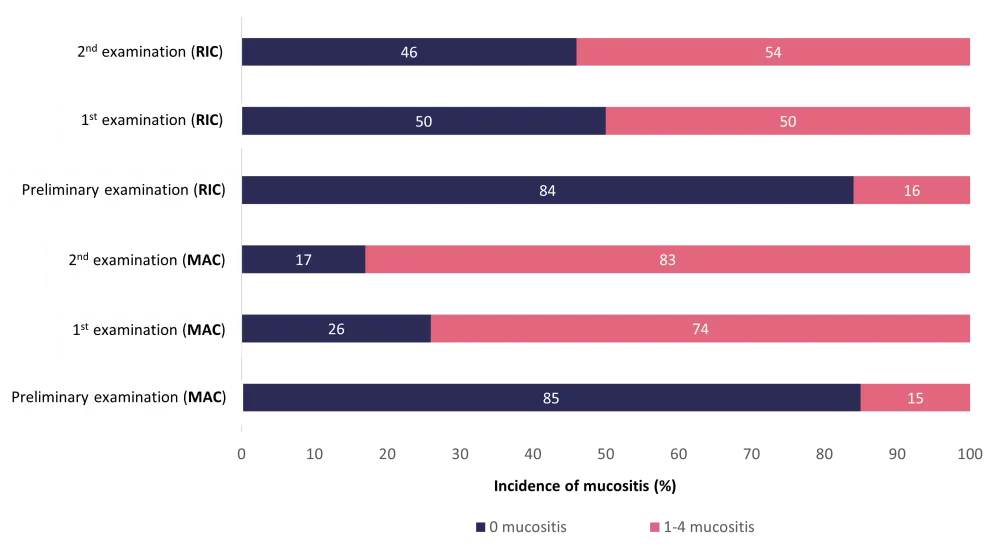
MAC, myeloablative conditioning; RIC, reduced intensity conditioning; WHO, World Health Organization.
*Adapted from Wysocka-Słowik et al.1
†Five-point scale recommended by the WHO.
- A statistically significant increase in the incidence of Grade 1 mucositis (p = 0.0002, p = 0.0240), Grade 2 mucositis (p = 0.0040, p < 0.0001), and Grade 3 mucositis (p = 0.0478, p = 0.0031) was observed at both first and second examinations, respectively, in the MAC group.
- Patients with Grade 3 mucositis increased after the first examination compared to second examination (7% vs 15%) in the MAC group, but decreased (4% vs 0%) in the RIC group, respectively, with a statistically significant difference between the two groups (p = 0.0372).
- Patients in the RIC group showed significant differences in the incidence of Grade 0 mucositis only between preliminary and first examination (p = 0.0091), and between preliminary and second examination (p = 0.0041).
- Patients in the MAC group demonstrated the highest mean value of the mucositis index 1.59 compared to 0.8 in the RIC group, with a significant increase in the mean value from preliminary to first examination in the MAC group.
- Parental nutritional therapy was given to three patients (MAC, n = 2; and RIC, n = 1) from the entire cohort; however, oral mucositis was not the only reason for inducing the nutritional therapy.
Conclusion
The study demonstrated that oral mucositis occurred less frequently and with lower intensity in patients with RIC therapy compared to MAC therapy. Quality of life due to oral mucositis is greatly reduced in patients with AML leading to premature termination of treatment. With the continuous growth of allo-HSCT as a treatment option for patients with AML, it warrants further investigation of oral mucositis in these patients.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?