All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Decitabine maintenance therapy benefits patients with CBF AML and persistent fusion transcripts at a low level after a FLAG-based regimen
Core-binding factor (CBF) acute myeloid leukemia (AML) is a subtype of AML, identified by the presence of t(8;21)(q22;q22) or inversion(16)(p13q22)/t(16;16) recurrent translocations, producing RUNX1/RUNX1T1 (AML1/ETO) or CBFB/MYH112 fusion transcripts, respectively.1
The presence of these transcripts allows for serial monitoring by real-time quantitative reverse transcription polymerase chain reaction (qRT-PCR) for detection of measurable residual disease (MRD). Senapati et al.1 studied decitabine (DAC) maintenance therapy with serial qRT-PCR to monitor MRD, after fludarabine/cytarabine/granulocyte-colony stimulating factor (G-CSF) (FLAG)-based induction and consolidation regimens; the results were recently published in the American Journal of Hematology, and we summarize the study below.
Study design
Samples of bone marrow for serial qRT-PCR and flow cytometry were collected from each patient every 3 months. An increase in qRT-PCR from <0.01% was considered a molecular relapse. All patients had received at least one cycle of decitabine maintenance therapy. The pre-treatment regimen was as follows:
- Induction regimen
- Fludarabine 30 mg/m2 on Days 1–5
- Cytarabine 2 g/m2 intravenous (IV) on Days 1–5
- Idarubicin 6 mg/m2 on Days 3–4
- G-CSF 5 mcg/kg on Day 1
- Gemtuzumab ozogamicin 3 mg/m2 on Day 1
- Consolidation therapy
- FLAG-based therapy for 3 days
- Gemtuzumab ozogamicin on Day 1 in Cycles 2/3 and 5/6 or with idarubicin
A total of 31 patients received monthly decitabine maintenance therapy at 20 mg/m2 on Days 1–5, every 4–5 weeks, based on count recovery and toxicity. For patients with concerning cytopenias the regimen was reduced to Days 1–3. The treatment and number of cycles for each group is shown in Figure 1.
Figure 1. Study design*
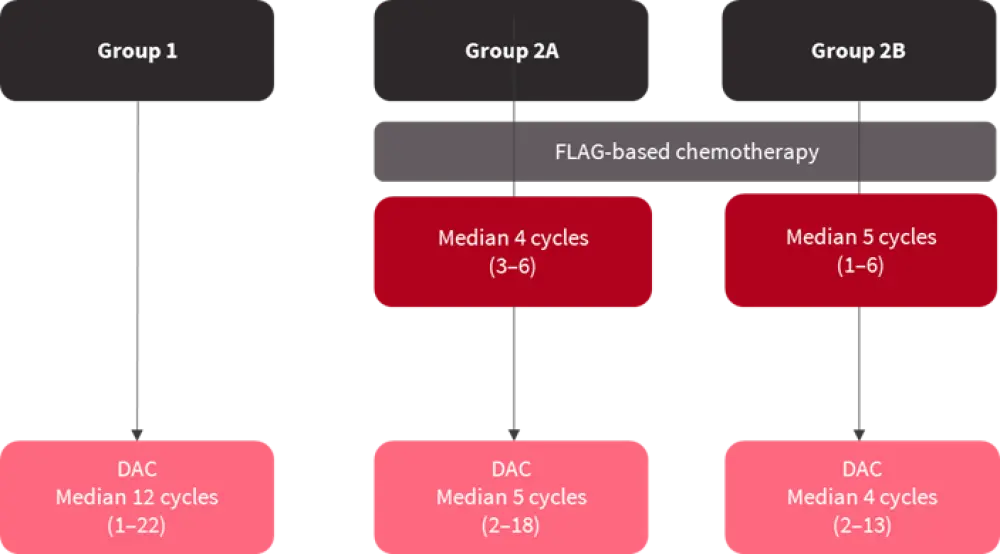
DAC, decitabine; FLAG, fludarabine, cytarabine, and granulocyte-colony stimulating factor.
*Adapted from Senapati et al.1
Results
Out of the 31 patients receiving decitabine therapy, 14 were identified to have the t(8;21) translocation and 17 patients with inversion(16). The median age of the cohort was 57 years old with a median follow-up time of 59.3 months.
Group 1
A total of 15 patients in this cohort received 12 cycles of decitabine maintenance therapy. 10 patients cleared their fusion transcripts; however, five patients never achieved complete molecular response (CMR) (qRT-PCR result of 0.56%), and one patient had a late molecular relapse, showing persistent low qRT-PCR values (<0.01%). The median follow-up time for the cohort was 71.5 months, with 14 patients still being alive. The median estimated overall survival (OS) rate was 114 months.
Group 2A
A total of eight patients were included in this group, receiving a median of four cycles of FLAG-based chemotherapy and a median of five decitabine maintenance cycles. Four patients received less than the standard 12 cycles of decitabine maintenance, and only two required salvage therapy after molecular relapse. The median follow-up time was 65.1 months with six patients still being alive. The estimated OS was 101.9 months.
Group 2B
For this group, all eight patients received less than seven cycles of FLAG-based chemotherapy and a median of four cycles of decitabine maintenance. The median qRT-PCR positivity was 0.1%. Two patients achieved CMR, and one patient had a 2-log reduction with decitabine therapy; all three patients subsequently had molecular relapses. All patients were initiated on second-line treatments with a median qRT-PCR result of 35.34%, and five patients proceeded to stem cell transplantation (SCT).
Survival and time to next treatment
Time to next treatment was considered an important endpoint for the study. The median time for each patient group is shown in Figure 2.
Figure 2. Median time to next treatment*
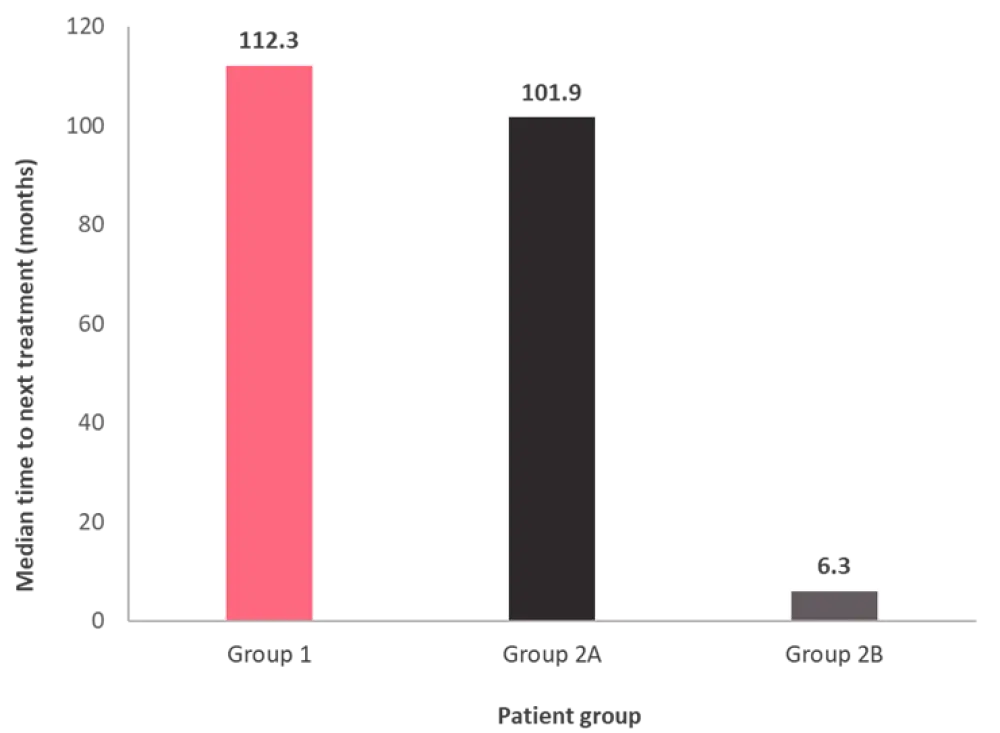
*Adapted from Senapati et al.1
For the 20 patients who achieved CMR, the median relapse-free survival was 94 months. The median follow-up time was 59.5 months. The OS for each group is shown in Figure 3. The median time for patients with CMR to next treatment was 112.4 months compared to 5.8 months for patients with no response. The OS for patients with a complete response was 116.3 months.
Figure 3. Overall survival rate*
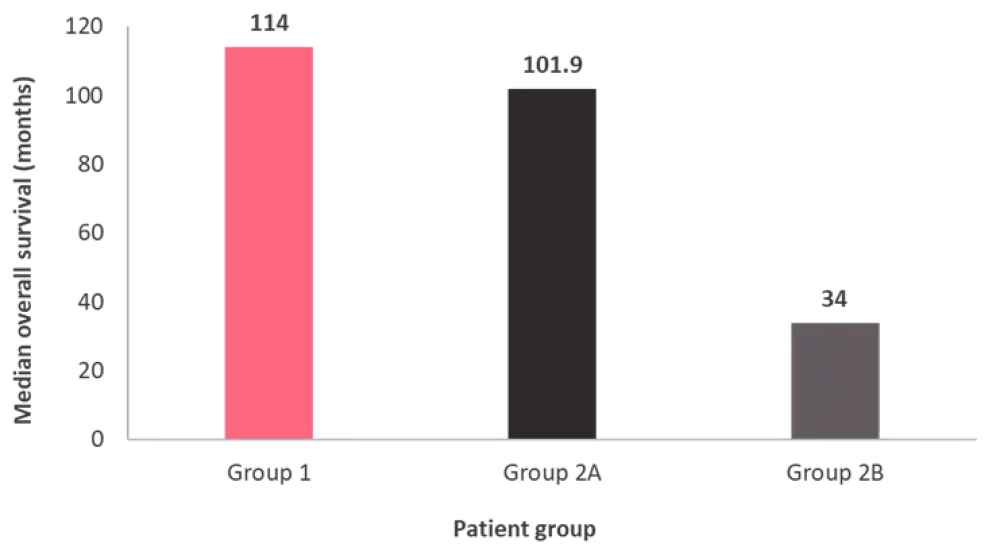
*Adapted from Senapati et al.1
All patients in Groups 1 and 2B (n = 23) had a positive pre-decitabine qRT-PCR result, with 12 patients achieving CMR at a median time of 7.4 months; of these patients, four experienced molecular relapses. The other 11 patients had no response, with three experiencing hematologic relapses.
Stem cell transplantation
A total of 10 patients underwent SCT, which includes three patients who went directly to transplantation due to molecular persistence, and the other seven received interim salvage therapy before transplantation. The median follow-up time after SCT was 42.9 months; at that point, eight patients were still alive with a negative qRT-PCR result. The median OS for this group was not reached.
Conclusion
The aim of decitabine maintenance therapy was to prevent or delay disease relapse. Patients unable to complete the desired consolidation therapy and/or who had persistent PCR transcripts achieved a long median relapse-free survival and salvage treatment-free remission. The patient cohort that received the full 12 recommended cycles of decitabine maintenance therapy, achieved the highest OS rate compared to patients who received a combination of decitabine and FLAG chemotherapy.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?