All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
DECIDER study: The addition of all-trans retinoic acid to decitabine improves survival in elderly patients with AML
Despite the availability of DNA hypomethylating agents (HMAs), the prognosis of unfit, older patients with acute myeloid leukemia (AML) is still poor. Approximately half of patients who receive HMA therapy respond to treatment, but even these responders are subject to secondary resistance and poor clinical outcomes. Drug combinations with histone deacetylase inhibitors (HDACi), BCL-2 inhibitors, or all-trans retinoic acid (ATRA) have been studied. In a previous publication, Michael Lübbert et al. reported the results of a non-randomized phase II study investigating decitabine in older, non-fit patients with AML (DRKS00000069). This trial had encouraging results, with good feasibility for patients treated with decitabine.
During the 25th European Hematology Association (EHA) Annual Congress, 2020, Michael Lübbert presented an abstract on the results from a four-arm, randomized phase II study, which investigated whether the addition of either valproic acid (VPA; HDACi activity) or ATRA or both to decitabine as first-line treatment for elderly patients with AML could be superior to decitabine alone (DECIDER study; NCT00867672).1
Study design
- This trial randomized 200 patients into four treatment arms with no crossover allowed
- DECIDER had a 2 × 2 factorial design, see Figure 1
Figure 1. The 2 × 2 factorial design of the phase II trial1
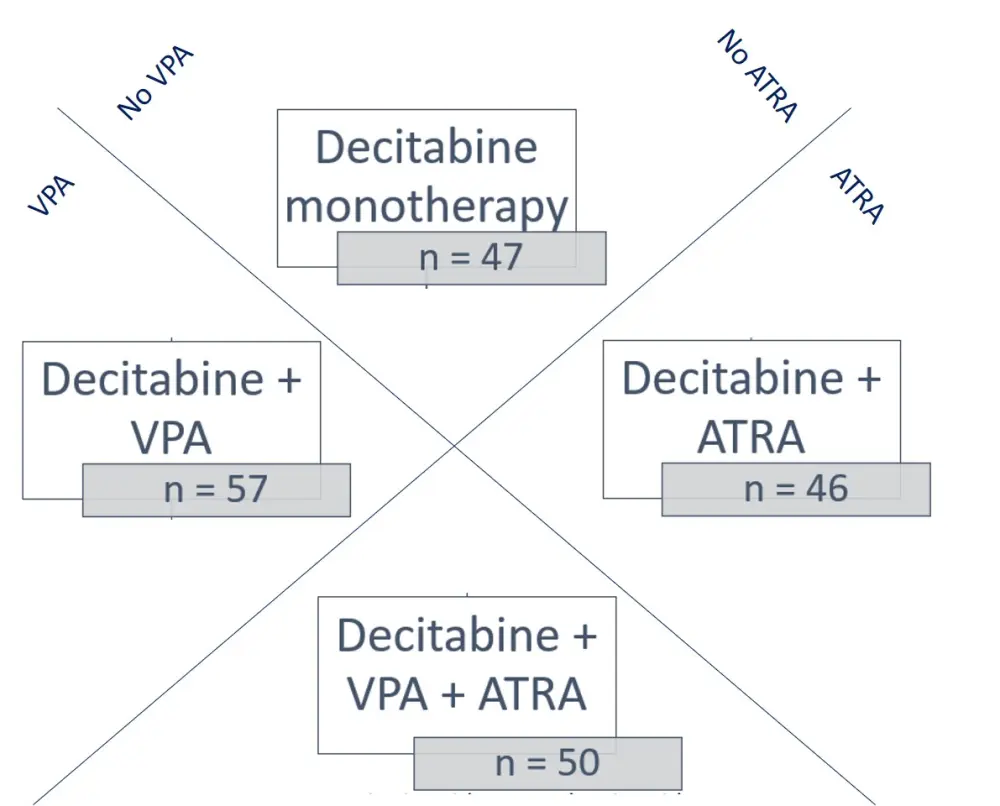
ATRA, all-trans retinoic acid; VPA, valproic acid
Dosing
The treatment course duration was 28 days, and a total of six courses were given with the option to continue with the same treatment:
- Day 1–5: decitabine (20 mg/m2)
- Day 6 and onwards: VPA (target serum levels of 80–100 ng/ml)
and/or
- Day 6–28: ATRA (45 mg/m2) daily
Inclusion criteria
- Aged ≥ 60 years old
- Primary or secondary AML, with no foreseeable benefit from standard induction chemotherapy
- Naive to AML treatment
- Performance status ECOG of 0–2
- Normal cardiac and kidney function
The key patient characteristics are shown in Table 1.
Key endpoints
- Overall response rate (ORR): complete remission, complete remission with incomplete hematologic recovery, and partial remission
- Secondary endpoints included overall survival (OS), progression-free survival (PFS), safety, quality of life, and nights in hospital
Table 1. The patient characteristics in all treatment arms1
|
AML, acute myeloid leukemia; ATRA, all-trans retinoic acid; ECOG, Eastern Cooperative Oncology Group; ELN, European LeukemiaNet; Int, intermediate risk; LDH, lactate dehydrogenase; VPA, valproic acid; WBC, white blood cells |
|||||
|
|
Total |
Decitabine |
Decitabine + VPA |
Decitabine + ATRA |
Decitabine + VPA + ATRA |
|---|---|---|---|---|---|
|
|
N = 200 |
n = 47 |
n = 57 |
n = 46 |
n = 50 |
|
Male gender, % |
64 |
66 |
67 |
61 |
62 |
|
Median age, years ≥ 80 years old, % |
76 21 |
75 19 |
76 14 |
77 26 |
77 26 |
|
ECOG performance status 2–3, % |
20 |
19 |
21 |
22 |
18 |
|
Comorbidities ≥ 3, % |
52 |
49 |
56 |
54 |
48 |
|
Prior hematological disorder, % |
51 |
53 |
47 |
54 |
50 |
|
Treatment-related AML, % |
14 |
13 |
14 |
20 |
8 |
|
Median WBC |
4.1 |
2.5 |
4.1 |
7.2 |
3.4 |
|
Serum LDH ≥ 300 U/L, % |
49 |
49 |
39 |
63 |
48 |
|
ELN genetics, % Good/Int-1 Int-2/Poor |
39 52 |
43 47 |
32 63 |
46 41 |
38 50 |
Results
The addition of ATRA resulted in a higher ORR (Table 2), therefore the primary endpoint was met.
Table 2. The overall best response rates per treatment arms1
|
ATRA, all-trans retinoic acid; VPA, valproic acid |
||||
|
|
Decitabine |
Decitabine + VPA |
Decitabine + ATRA |
Decitabine + VPA + ATRA |
|---|---|---|---|---|
|
Best response, % |
8.5 |
17.6 |
26 |
18 |
- No change in ORR was observed with VPA (17.8%) or without VPA (17.2%) (OR, 1.06; 95% CI, 0.51–2.21; p = 0.88)
- The ORR was significantly higher following the addition of ATRA (21.9%) vs no ATRA (13.5%) (OR, 1.80; 95% CI, 0.86–3.79; p = 0.12)
- OS was not influenced by the addition of VPA. The median OS was 6.2 vs 6.4 months in the VPA vs no VPA arms (multivariate analysis: HR, 0.97; 95% CI, 0.70–1.34; p = 0.84)
- The addition of ATRA significantly prolonged OS. The median OS was 8.2 vs 5.1 months in patients who received ATRA vs no ATRA (multivariate analysis: HR, 0.61; 95% CI, 0.44–0.84; p = 0.003)
- The benefit of adding ATRA was seen across different risk groups, including patients with adverse-risk genetics
- The addition of VPA did not influence PFS (HR, 0.89; 95% CI, 0.65–1.21; p = 0.46), whereas the addition of ATRA significantly improved PFS (HR, 0.66; 95% CI, 0.48–0.90; p = 0.009)
- To explore why the addition of ATRA resulted in clinically significant extension of survival, the authors performed an Aalen-Johansen estimator analysis:
- ATRA prolonged the time that patients maintained a response, which was not observed with VPA
- Analysis of conditional survival after response attainment showed that the addition of ATRA was beneficial vs no ATRA (HR, 0.65; 95% CI, 0.36–1.19), while VPA did not confer any benefit (HR, 1.12; 95% CI, 0.66–1.90)
- Survival without response (either with stable disease or progressive disease) was improved with ATRA add-on, but not with VPA add-on
- The addition of ATRA also improved the conditional survival from treatment failure (HR, 0.62; 95% CI, 0.39–0.98), while VPA add-on continued to have no effect (HR, 0.95; 95% CI, 0.62–1.47)
Conclusion
The addition of ATRA, but not VPA, to decitabine improved the ORR, OS, and PFS of elderly patients with AML, without additional safety concerns. The ATRA-mediated survival extension was seen across different patient subsets, including those with adverse-risk cytogenetics. Patients treated with the addition of ATRA were able to maintain response for a longer time. This was not only seen in patients who achieved an objective response, but also in those with stable or progressive disease. Additional studies that make use of mutational profiling to analyze potential outcome associations are needed to better understand the underlying genetics and epigenetics, particularly in such patients who are likely to develop HMA resistance.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?