All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View AML content recommended for you
A proposed molecular framework for disease classification and risk stratification in AML
Do you know... Using comprehensive molecular profiling, a recent study characterized and validated 16 molecular classes describing AML patients. Which molecular class has been associated with the highest salvage frequencies, as compared to all other AML classes?
Classification and risk-stratification in acute myeloid leukemia (AML) relies on cytogenetic findings at diagnosis and informs treatment decisions. With the increased use of prospective sequencing during AML diagnosis, understanding the role of molecular and genetic biomarkers in the conventional endpoints such as minimal residual disease (MRD), complete remission (CR), and relapse is essential. There is also a need for evidence-based clinical decision support tools that integrate genetic, molecular, and clinical biomarkers to optimize diagnosis and treatment decisions.1
Below, we summarize a recent study by Tazi, et al.,1 published in Nature Communications, investigating a unified framework for classification and risk-stratification in AML using cytogenetics and the development of an open-access, patient-tailored, clinical decision support tool.
Study design and methods
This was a retrospective, cohort study, using real-world patient data from UK National Cancer Research Institute (UK-NCRI) clinical trials in adult patients with AML who were eligible for intensive or non-intensive treatment (AML-NCRI). The validation cohort included patients with AML from the AML study group (AML-SG) with comparable molecular features at diagnosis. The study design and methods are shown in Figure 1.
Figure 1. Study design and methods*
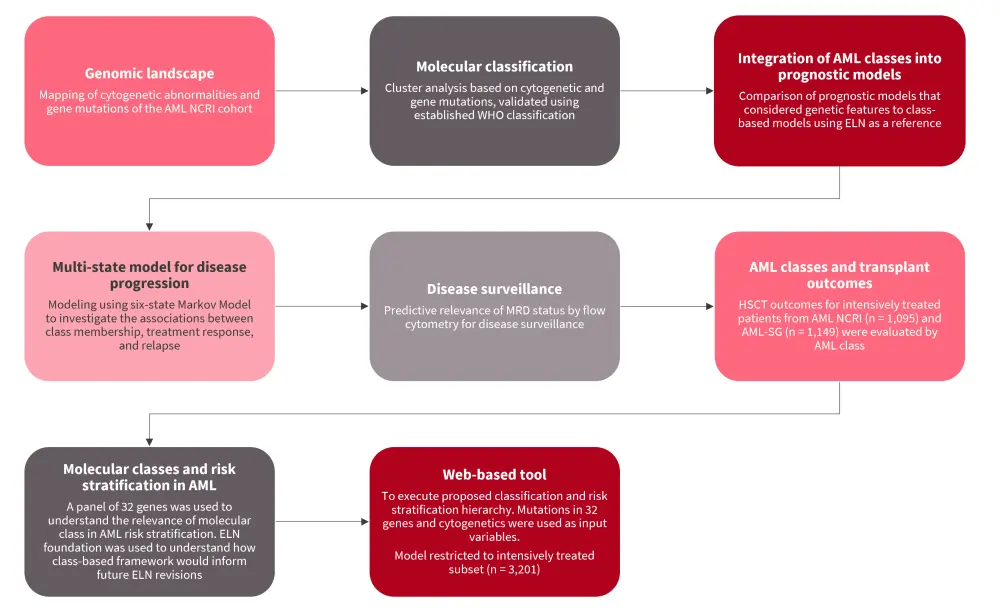
AML, acute myeloid leukemia; CR, complete remission; ELN, European Leukemia Network; HSCT, hematopoietic stem cell transplantation; MRD, minimal residual disease; NCRI, National Cancer Research Institute; SG, study group; WHO, World Health Organization.
*Adapted from Tazi, et al.1
Results
A total of 2,113 and 1,540 patients with AML were included in the AML-NCRI and AML-SG cohort, respectively.
Genomic landscape
Overall, there were 8,460 driver events occurring in the AML-NCRI cohort based on mapping of cytogenetic abnormalities and mutations. Detailed examination of the genotype and clinical relationships of 70 well-established recurrent cytogenetic abnormalities and 84 genes in the AML-NCRI cohort revealed consistency with previous studies.
Molecular classification
Nearly half (49.6%) of patients from the AML-NCRI cohort were mapped based on World Health Organization (WHO) 2016 classification.
- Overall, 14 non-overlapping clusters classifying 92% of patients validated the established WHO entities and confirmed previously uncharacterized molecular subgroups which accounted for 33.3% of patients with AML.
- Heterogeneity in patients with AML at diagnosis across age, peripheral blood, and blast count was explained by the distinct demographic and clinical parameters of each class.
Classes by cytogenetic alterations included entities defined by translocations and patients with complex karyotype, who frequently (65%) had TP53 mutations.
- Complex karyotype was characterized by older age (median age at diagnosis, 62 years) and poor outcomes.
- A novel cytogenetic group (11.2%) was defined by the presence of ≥1 trisomies, frequently involving +8, +11, +13, +21, and +22 without any deletions, and associated with favorable disease, even in the presence of ≥3 trisomies.
- Patients from the second largest cluster (28.4%), defined by ≤2 aneuploidies (11%) enriched for MDS cytogenetic abnormalities + secondary AML (sAML) mutations (28.4%), were older, had lower blast counts, and higher incidence of antecedent hematologic disease (AHD).
- Patients in this group were subgrouped into secondary AML Like-1 (sAML1), defined by single mutations (n = 100), and secondary AML Like-2 (sAML2), defined by ≥2 class-defining genes (n = 501).
- Patients with sAML2 had poorer 5-year survival rate of 16% compared to those with sAML1 (37%). AHD was more common in sAML2 subgroup and was associated with worse outcomes.
- The provisional WHO entity (RUNX1) spread across both sAML1 and sAML2 subgroups without conferring an independent prognosis.
- The presence of WT1 mutations with no other classifying events led to a separate group where patients had a lower number of mutations and intermediate-risk disease in the absence of FLT3 mutations, were younger at diagnosis, and had higher white blood cell counts.
- The DNMT3A/IDH subgroup (1%) was defined as a heterogeneous group.
- Six percent of patients that did not cluster with any class were labeled as molecularly not otherwise specified and 2% of patients had no identifiable mutations.
These findings informed a hierarchical classification (Figure 2) and assigned 100% of patients into molecular class (total of 16 classes). sAML1, sAML2, WT1, and trisomy classes defined the independent prognostic groups relative to European Leukemia Network (ELN). Most patients under the new hierarchy had intermediate-risk AML, and patients with no mutations had favorable outcomes. The associations of these subgroups remained consistent in the validation cohort. Fms-like tyrosine kinase 3 (FLT3) mutations were present across the classes and were therefore not class defining.
Figure 2. Hierarchical AML classification schema*
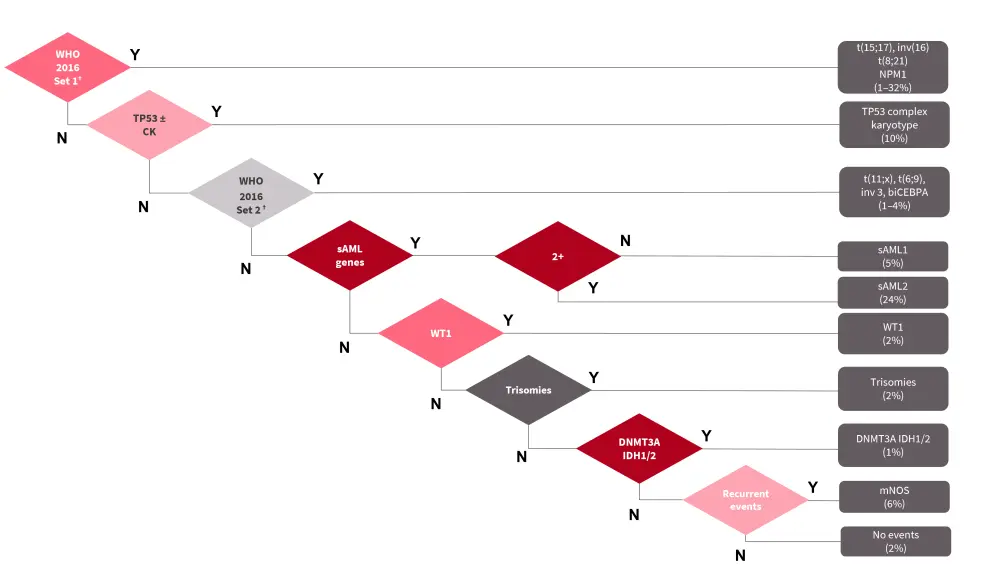
AML, acute myeloid leukemia; biCEBPA, biallelic CCAAT enhancer binding protein alpha; CK, complex karyotype; DNMT3A/IDH2, deoxyribonucleic acid methyltransferase 3A/isocitrate dehydrogenase 2; mNOS, molecularly not otherwise specified; NPM1; nucleophosmin 1; sAML1, secondary AML Like-1; sAML2, secondary AML Like-2; TP53, tumor protein 53; WHO, World Health Organization; WT1, Wilms tumor 1.
*Adapted from Tazi, et al.1
†WHO Set 1 included (15;17), inv(16),t(8;21), and NPM1; WHO Set 2 included t(11;x), t(6;9), inv 3, and biCEBPA.
Integration of AML classes into prognostic models
When models incorporating genetics and those considering AML classes were compared, a simple model of AML class and FLT3ITD status captured the same information as more complex genetic models. This demonstrates a need for novel risk-stratification schema based on these parameters.
Inclusion of clinical features such as age, AHD, performance status, white blood cells (WBCs), hemoglobin, and platelet attained the highest improvement in model bias and were comparable in the validation cohort. This observation indicates the generalizability of the classification.
Multi-state model for disease progression
This analysis focused on the associations between AML class, treatment response, and relapse. The detailed analysis of the transition between two clinical endpoints (e.g., alive in CR to death in CR) over time resulted in survival estimates of anticipated transitions across molecular subgroups (Figure 3). These observations were also confirmed in the validation cohort.
Taken together, the findings characterize classes that were previously grouped as heterogenous or intermediate-risk groups; this provides further insight into patients’ response to treatment, the risk of disease progression, relapse, and death.
Figure 3. Patient transitions and outcomes*
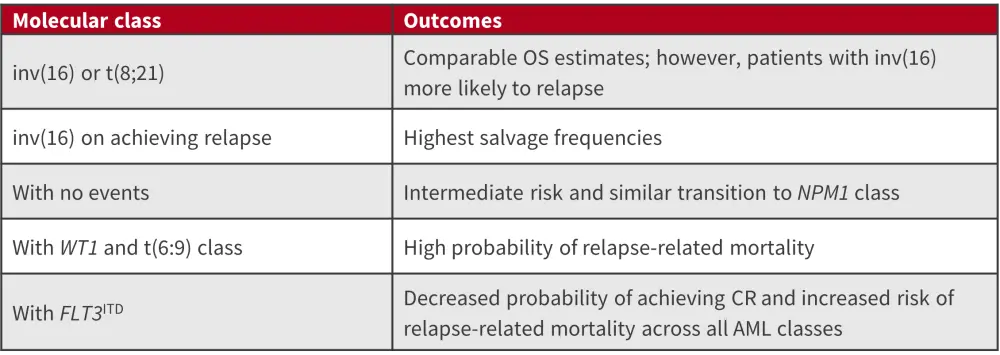
AML, acute myeloid leukemia; CR, complete remission; FLT3ITD, Fms related receptor tyrosine kinase 3 internal tandem duplicates; OS, overall survival; WT1, Wilms tumor 1.
*Adapted from Tazi, et al.1
This analysis also demonstrated that responses to induction chemotherapy provided a distinction between sAML1 and sAML2 subgroups. A higher proportion of patients in the sAML2 subgroup did not attain CR compared with the sAML1 subgroup following induction chemotherapy (43.7% vs 26%, p = 0.002). Adverse outcomes observed in TP53/complex and inv(3) were mainly due to highly chemoresistant disease and relapse-related mortality.
Implications for disease surveillance
Data on MRD status was available from 523 patients in the AML-NCRI cohort; 202 were negative (MRD−) and 321 were MRD positive (MRD+).
- In the sAML2 subgroup, nearly 70% of patients in CR with MRD+ status showed no significant difference in relapse and survival rates, or no difference of effect by group (p = 0.3).
- Similarly, patients in the sAML1 group showed no difference in the incidence of relapse in both MRD− or MRD+ patients.
The findings indicate that MRD− status may not be universally applicable across classes due to differences in the underlying biology associated with mutations in each class.
AML classes and transplant outcomes
Investigators also investigated the hematopoietic stem cell transplantation (HSCT) outcomes based on AML class.
- Patients in the sAML2 subgroup undergoing HSCT had a reduced risk of death, following adjustment for performance status and age (p < 0.0001), but there was no significant survival difference based on patients undergoing HSCT in CR1 or CR2.
- Patients with TP53 complex karyotype (CK) also benefitted from HSCT; however, patients with TP53-CK transplanted in CR2 had significantly worse survival rates than those transplanted in CR1 (p = 0.009).
- Similarly, patients in the sAML1 subgroup undergoing HSCT in CR1 benefited compared with CR2.
Molecular class in AML risk stratification
To evaluate whether this proposed framework would inform upcoming ELN revisions, patients were assigned to each of the three proposed risk strata using the ELN framework (Figure 4). Updated ELN 2022 recommendations regarding the diagnosis and classification of AML in adult patients can be found here. According to ELN classification, t(6;9) was considered an adverse risk group; however, the new risk stratification showed that adverse risk is specific to the subset of patients with FLT3ITD. It also highlighted FLT3ITD as the only mutation that delivers independent prognostic information from class membership and was associated with worse outcomes for all intermediate-risk classes. The stratification therefore used FLT3ITD status to upgrade risk for all intermediate-risk patients to adverse risk.
The new framework re-stratified 25.5% and 24.6% of patients from AML-NCRI and AML-SG cohort, respectively. Although there was an overlap with ELN trajectories, the new framework led to a significant improvement in the concordance-index (AML-NCRI, p = 0.05; AML-SG, p = 0.025).
Figure 4. New risk stratification based on AML classes*
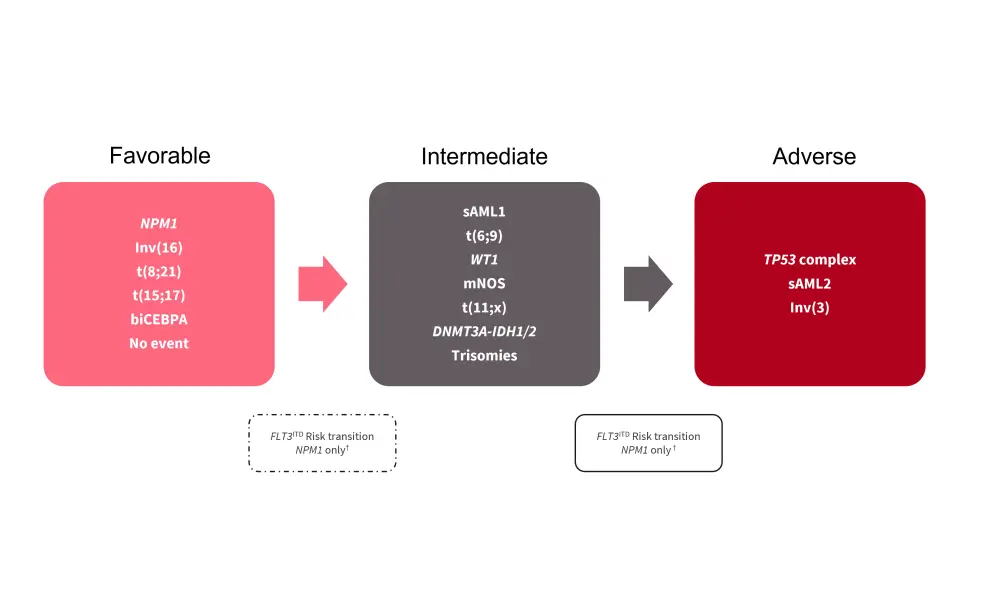
AML, acute myeloid leukemia; biCEBPA, biallelic CCAAT enhancer binding protein alpha; DNMT3A/IDH, deoxyribonucleic acid methyltransferase 3A/isocitrate dehydrogenase; FLT3, Fms-like tyrosine kinase 3; mNOS, molecularly not otherwise specified; NPM1, nucleophosmin 1; sAML1, secondary AML Like-1; sAML2, secondary AML Like-2; TP53, tumor protein 53; WT1, Wilms tumor 1.
*Adapted from Tazi, et al.1
†The dotted box refers to the risk transition for patients with both NPM1 and FLT3ITD mutations from favorable to intermediate. The solid box refers to the risk transition for patients with FLT3ITD from intermediate to adverse.
Clinical decision support tool
This web-based tool executes the new classification and risk stratification hierarchy based on mutations in 32 genes and cytogenetics; the model is restricted to an intensively treated subset of patients (n = 3,201) which accounted for 90% in both the AML-NCRI and AML-SG cohorts. End-point specific predictions over time are represented as sediment and bar plots. The tool contains a tab to include patient specific covariates that inform each transition estimate along with corresponding coefficients. It also contains a warning sign for outlier cases and computes confidence intervals for all predictions.
Conclusion
This cohort study using comprehensive analyses and a validation cohort provides a unified framework for the classification and risk stratification in AML. The new framework classified 100% of included patients into one of 16 molecular subgroups. This new framework facilitates an improved understanding of novel and established cases. Although there were differences in clinical trials and demographics between the test and validation cohort, the molecular classes captured the spectrum of phenotypic and clinical heterogeneity; this demonstrates the generalizability of the findings. However, further studies focused on investigating class association with MRD status and responses to emerging therapies, including combination regimens, are needed.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?