All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Quantifying patient and physician preferences in post-HSCT maintenance treatment of AML
Hematopoietic stem cell transplant (HSCT) in patients with acute myeloid leukemia (AML) is often followed by maintenance therapy to prolong remission. Currently, there are no universally accepted standard maintenance therapies, leaving patients and physicians to determine which treatment to use by assessing the risk/benefit of the different options available. A better insight into why certain treatments are selected, how these risks/benefits are weighed by patients and physicians, and any impact of either group preference on the other, could be valuable. Ultimately, this could lead to a better selection of treatments and improve treatment satisfaction in patients.
Manasee Shah and colleagues,1 investigated these preferences for post-HSCT treatment of AML using a discrete choice experiment (DCE). DCE is a robust method used to capture the preferences of individuals for different health technologies, enabling an estimate of the relative importance of different treatment attributes. The investigators used this method to quantify preferences for post-HSCT maintenance treatment of AML, to determine what treatment attributes are important to both patients and physicians. The results were presented at the 26th Congress of the European Hematology Association (EHA2021) and are summarized below.
Study design and patients1
- Targeted literature review and telephone interviews (one-to-one) with four physicians and six patients informed the post-treatment attributes used in the DCE.
- Physicians who treat AML and patients with AML who had undergone HSCT were recruited in the US, UK, Canada, and Australia to complete a web-based DCE.
- Participants were asked to choose between two hypothetical treatment profiles with six attributes which varied between treatments (Figure 1). Attributes included:
- Chance of 2-year relapse-free survival (RFS)
- Average quality of life (QoL)
- Risk of serious infection
- Risk of nausea
- Chance of achieving transfusion independence
- Duration of hospitalization per year
- Conditional logit regression models were used to estimate preference weights and assess how treatment attributes impact the treatment choice.
- A total of 78 patients and 145 physicians completed the DCE, see Table 1.
Figure 1. Example of a DCE choice card*
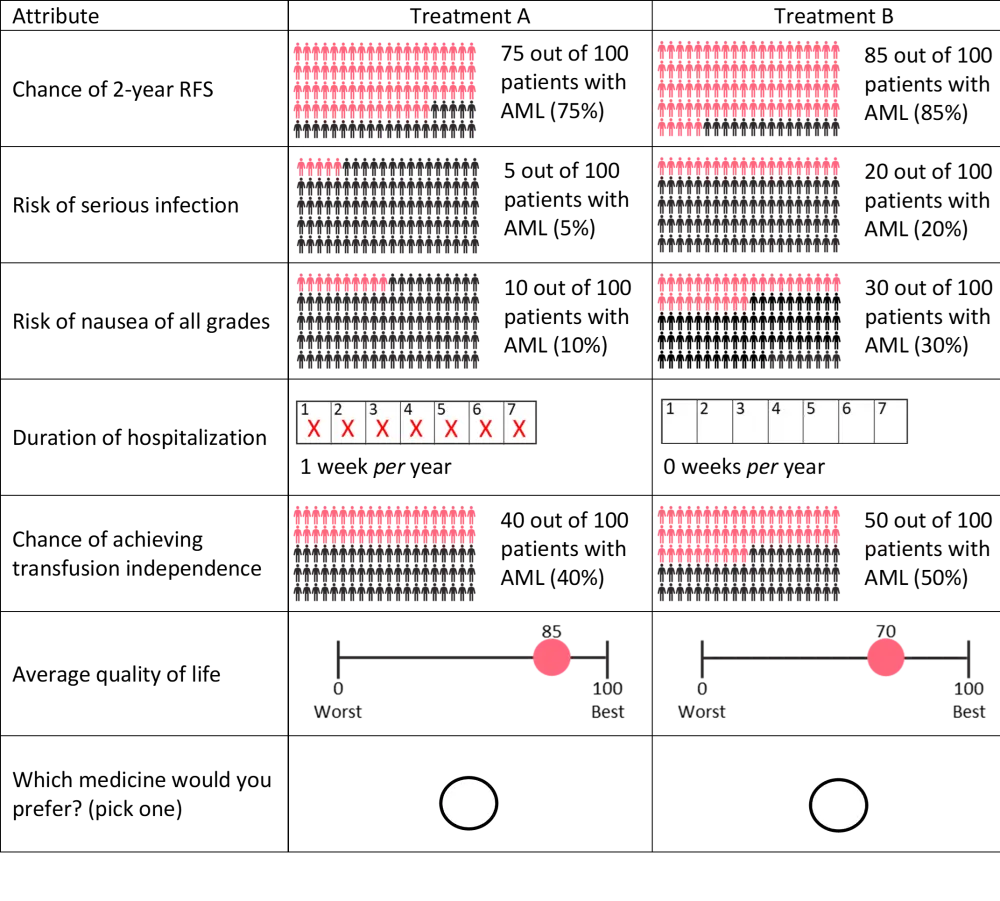
AML, acute myeloid leukemia; RFS, relapse-free survival.
*Adapted from Zhou et al.1
Table 1. Participant characteristics*
|
AML, acute myeloid leukemia; HSCT, hematopoietic stem cell transplantation; NA, not applicable; NR, not reported; SD, standard deviation. |
||
|
Characteristic |
Patients |
Physicians |
|---|---|---|
|
Age, years, mean (SD) |
62.0 (11.6) |
50.1 (8.3) |
|
Male, % |
59.0 |
75.9 |
|
Country, % |
||
|
US |
59.0 |
33.1 |
|
UK |
38.5 |
35.9 |
|
Canada |
2.6 |
20.0 |
|
Australia |
0 |
11.0 |
|
White, % |
52.6 |
NR |
|
Time since AML diagnosis, months, mean (SD) |
34.0 (28.9) |
NA |
|
Years practicing medicine, mean (SD) |
NA |
19.8 (7.4) |
|
AML patients treated in a typical year, mean (SD) |
NA |
47.7 (88.9) |
Results1
Based on preference weights determined during the DCE, the average QoL was the most important attribute in the selection of a maintenance treatment for patients with AML, followed by duration of hospitalization, and chance of 2-year RFS. For physicians, chance of 2-year RFS was the most important attribute, followed by average QoL, and risk of serious infections. Patient and physician attribute preference weights were not statistically compared. Patients were prepared to consider a less effective treatment if it improved QoL and if there was a reduction in hospitalization. Analysis found that a reduction in hospitalization of 2 weeks per year, or an improvement in QoL of 35 (on a 0−100 scale) each compensated for a 30% reduction in the 2-year RFS in the patient group. Duration of hospitalization and chance of achieving transfusion independence were both found to be less important to physicians than patients. Analysis of the physician group found that a reduction in hospitalization of 2 weeks per year compensated for a 10% increased risk of nausea or a 5% increased risk of serious infection.
Conclusion1
There were differences between the attributes deemed to be important between patients and physicians when selecting post-HSCT maintenance therapy. Although both groups valued QoL, physicians valued duration of hospitalization less than patients. The use of online panel-based surveys may have led to limitations around generalizability and selection bias, and the preference assessment was limited by the treatment attributes that were included. However, the study highlights the importance of conversations between physicians and patients to fully understand patient treatment goals and preferences when determining the post-HSCT maintenance treatment. Acknowledging the differences between physician and patient treatment preferences will enable physicians to better select patient-centered treatments.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?