All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Neutralizing antibody responses to SARS-CoV-2 in patients with AML or MDS
Do you know... In a recent study, neutralizing antibody responses to vaccine-homologous SARS-CoV-2 WA1/2020 strain were evaluated in patients with AML or MDS. Compared to healthy individuals, neutralizing antibody responses in patients with AML or MDS following two vaccinations were:
Severe acute respiratory syndrome coronavirus 2 (SARS-Cov-2) represents an increased risk for patients with immune dysfunction despite vaccination. This is commonly seen in patients diagnosed with hematologic malignancies, including acute myeloid leukemia (AML), and myelodysplastic syndromes (MDS). Breakthrough infections and complications as a result of immune dysfunction are a key contributor to patient mortality associated with these conditions.1
Despite this fact, there is currently an under representation in published studies regarding antibody neutralization after vaccination against the ancestral strain and variants of concern. In response to this, Lorenza Bellusci and colleagues1 performed SARS-CoV-2 virus neutralization assays to ascertain levels of neutralization of SARS-CoV-2 Omicron variant, after vaccination in patients with AML or MDS.1 We summarize the findings below.
Study design
A total of 48 patients, with a median age of 70, diagnosed with myeloid neoplasms and receiving standard care were included in the study. A separate group of 16 healthy healthcare workers with a median age of 34.5 years, neither exposed to nor having worked with COVID-19 patients, were used as the control. Neutralizing antibody responses to vaccine-homologous SARS-CoV-2 WA1/2020 strain and five variants of concern (VOCs) in the periods following second and third vaccinations, were evaluated using SARS-CoV 2 neutralization assays. The median time intervals between vaccination and evaluation of sera for the two groups were:
- Myeloid neoplasms group
- 150.5 days after the second vaccination (n = 38)
- 30.5 days after the third vaccination (n = 11)
- Control group
- 38 days after the second vaccination (n = 16)
- 57.5 days after the third vaccination (n = 16)
Results
After two vaccinations, the control group showed a strong response against the vaccine homologous WA1/2020. In contrast, patients with myeloid neoplasms recorded significantly weaker responses. There was no significant difference in response after two vaccinations between patients with AML or MDS. After three vaccinations, the control group consistently recorded strong neutralization antibody responses. Comparatively, 11 patients from the myeloid neoplasm cohort showed highly variable neutralization responses. Two patients from this cohort showed no response at all, and only four patients recorded strong neutralization responses. The change in geometric mean titers for both patient groups after Vaccinations 2 and 3 is shown in Figure 1.
Figure 1. Change in geometric mean titers for both cohorts after SARS-CoV-2 Vaccinations 2 and 3*
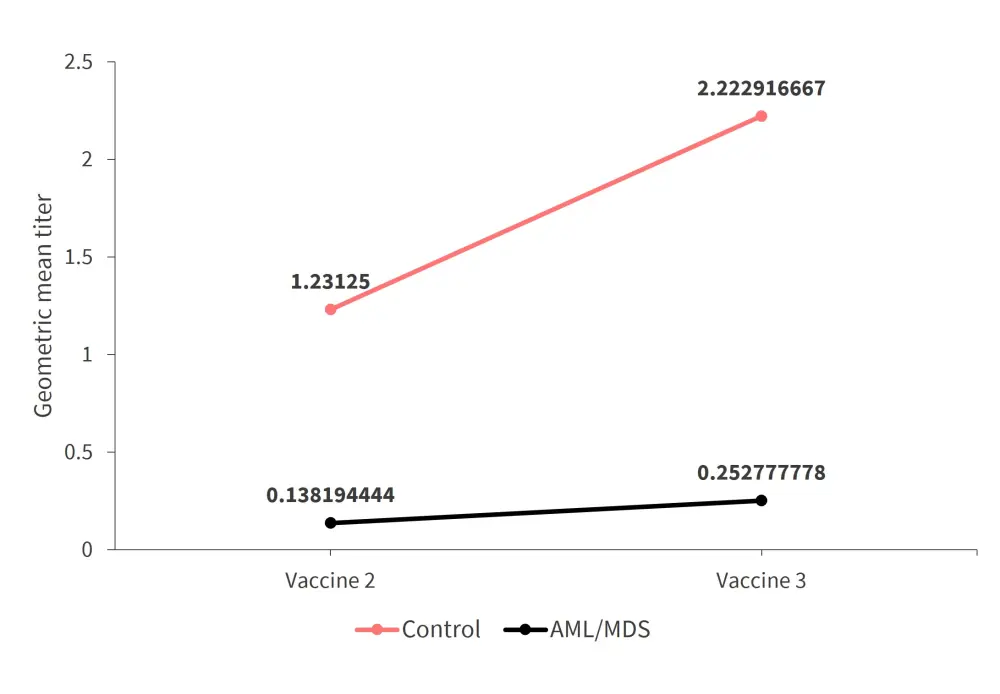
*Adapted from Bellusci et al.1
The control group showed similar fold reductions of activity against all variants and a more noticeable reduction against Omicron. Full results are shown in Figure 2.
Figure 2. Reduction of activity against SARS-CoV-2 variants of concern in healthy individuals after two vaccinations*
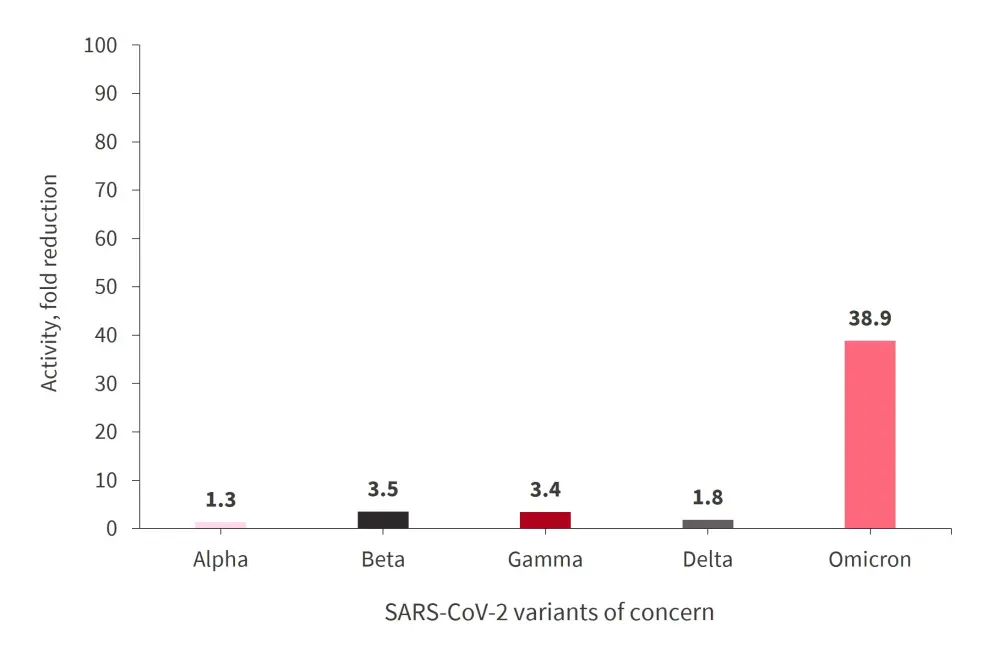
*Adapted from Bellusci et al.1
After three vaccinations, there was a modest increase in neutralization titers against each of the variants. In contrast, the majority of patients in the myeloid neoplasm cohort showed limited or no antibody response against all variants after two vaccinations. A total of seven patients showed limited responses after three vaccinations, whereas the remaining four recorded a strong response against the original strain but had a lower response against Omicron.
Since the low neutralization titers in the myeloid neoplasm group against both WA1/2020 and VOCs did not provide a full picture of antibody response to vaccination, the study also evaluated IgG binding to the SARS-CoV-2 spike receptor-binding domain (RBD) derived from the vaccine-homologous WA1/2020, as well as the Omicron variant, using the enzyme-linked immunosorbent assay (ELISA). Within the healthy cohort, a robust binding to both WA1 (original) and Omicron strains was detected after Vaccinations 2 and 3. However, patients with myeloid neoplasms showed more varied binding activity after the third vaccination. A total of 11 out of 38 patients from this group recorded RBD-IgG end-point titers below 1:200 serum dilution against Omicron. Furthermore, after receiving three vaccinations, this cohort showed increased antibody-binding titers against the Omicron RBD, although still lower than the control group.
Conclusion
Results from the study1 show that healthy individuals who have received three vaccinations are likely to be protected from severe COVID-19, but the effectiveness of two vaccine doses in patients with myeloid neoplasms is significantly reduced. Mass vaccination in Israel has shown 1.7 to 2.3 increased risk of symptomatic disease, hospitalization, and death for those with hematologic neoplasms. These observations highlight the immunodeficiency in this patient population, who are therefore likely to be at an increased risk of breakthrough infections. The authors recommended that post-exposure treatments after infection should now be the focus for patient care.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?