All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Low-dose chemotherapy regimen in de novo pediatric AML
The standard treatment for pediatric de novo acute myeloid leukemia (AML) treatment includes intensive chemotherapy for remission induction, followed by remission maintenance with intensive chemotherapy and/or hematopoietic stem cell transplantation (HSCT). Although progress has been made in reducing early death rates and overall treatment-related mortality (TRM), long-term effects of intensive chemotherapy in conjunction with deficient supportive care and stagnant overall survival (OS) rates remain a cause of concern, especially in low- and middle-income countries (LMICs).
TRM, leaving treatment early, or refusal to take treatment are the most common reasons in the early phases of AML treatment in the pediatric population and, therefore, may benefit from adjustments to the treatment regimen. In a recently published study, Hu et al. investigated the long-term impact of low-dose chemotherapy (LDC) vs standard-dose chemotherapy (SDC).1
Study design
An observational case control study in children aged ≤15 years with de novo AML (according to the World Health Organization criteria). A total of 183 patients were included and allocated to either LDC (n = 83) or SDC (n = 100) groups; as shown in Figure 1. Both groups received similar postremission consolidation therapy.
The primary endpoints were OS, event-free survival (EFS), and cumulative incidence of relapse (CIR).
Figure 1. Dosing schedule*
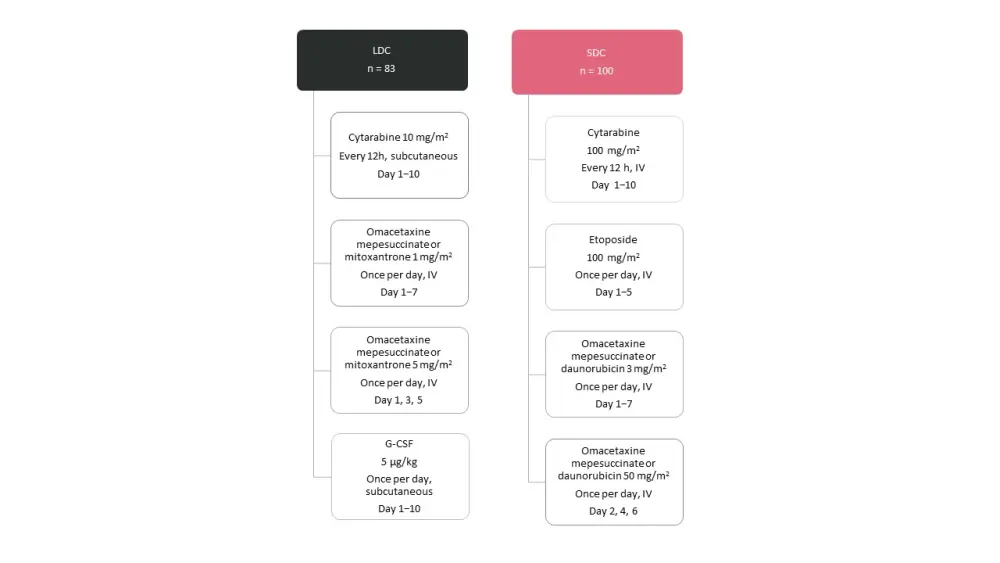
G-CSF, granulocyte-colony stimulating factor; IV, intravenous; LDC, low-dose chemotherapy; SDC, standard-dose chemotherapy.
*Figure adapted from Hu et al.1
Results
The baseline characteristics were comparable in both groups (as seen in Table 1). Patients in the SDC group had significantly higher white blood cell (WBC) count at the time of diagnosis, with a median of 27.7 (range, 0.42−606). A greater number of patients were classified as having high-risk AML in the SDC group (n = 37) compared with the LDC group (n = 16).
Table 1. Baseline characteristics*
|
LDC, low-dose chemotherapy; SDC, standard-dose chemotherapy; WBC, white blood cells. |
|||
|
Characteristic |
LDC |
SDC |
p value† |
|---|---|---|---|
|
Sex, % |
|
|
|
|
Age, median (range) |
6.1 (0.8–14.2) |
7.5 (0.3–13.8) |
0.424 |
|
WBC count, × 109/L, median (range) |
12.5 (1.33–283.41) |
27.7 (0.42–606) |
0.001 |
|
Gene rearrangements, % |
|
|
0.432 |
|
Gene mutations, % |
(n = 76) |
(n = 92) |
0.168 |
|
Provisional risk group, % |
|
|
0.035 |
|
Definitive risk group, % |
(n = 77) |
(n = 95) |
0.016 |
Efficacy and safety
Induction response
- Responses after first induction in both LDC and SDC groups were similar, with complete remission (CR) observed in 70% vs 67% in the LDC and SDC groups, respectively (see Table 2).
Table 2. Induction responses*
|
CR, complete remission; LDC, low-dose chemotherapy; NR, nonresponse; PR, partial remission; SDC, standard-dose chemotherapy; TRM, treatment-related mortality. |
|||
|
Response |
LDC |
SDC |
p value |
|---|---|---|---|
|
First induction, % |
|
|
0.811 |
|
Second induction, % |
(n = 80) |
(n = 96) |
0.436 |
|
TRM, n |
1 |
2 |
1.000 |
|
Dropouts, n |
7 |
7 |
0.912 |
Postremission consolidation
- The overall response rate (ORR) was similar in both groups, with 21% (17/83) of relapses in the LDC group and 16% (16/100) in the SDC group (p = 0.447).
- 46% (38/83) of patients in the LDC group received HSCT compared with 48% (48/100) in the SDC group (p = 0.76).
Survival and prognostic factors
- The median follow-up was 50 months (range, 4−85 months). The multivariable regression analysis showed that there was no significant impact from induction treatment on OS, EFS, and CIR (see Table 3). However, HSCT was significantly associated with OS (hazard ratio [HR], 0.39; p = 0.007), as well as the definitive risk classification (SDC, 25 vs LDC, 6 recipients; p = 0.01).
- The 5-year EFS in the LDC and SDC groups was 61% ± 9% and 65% ± 7%, respectively (p = 0.462); OS was 73% ± 7% vs 73% ± 6 (p = 0.933); and CIR was 21% ± 5% vs 18% ± 4% (p = 0.484).
- No significant differences were seen in patients with a WBC count of < 100 × 109/L in either the LDC group or SDC group for OS (73% ± 5% vs 80% ± 5%, respectively; p = 0.332) or EFS (61% ± 6% vs 70% ± 5%, respectively; p = 0.17).
Table 3. Multivariable COX regression of OS, EFS, and CIR*
|
CI, confidence interval; CIR, cumulative incidence rate; EFS, event-free survival; FAB, French- American-British; HSCT, hematopoietic stem-cell transplantation; HR, hazards ratio; LDC, low-dose chemotherapy; OS, overall survival; SDC, standard-dose chemotherapy; WBC, white blood cells. |
|||
|
Factor |
OS |
EFS |
CIR |
|---|---|---|---|
|
HR (95% CI; p value) |
HR (95% CI; p value) |
HR (95% CI; p value) |
|
|
WBC, × 109/L, |
|
|
|
|
FAB subtype |
|
|
|
|
Definitive risk |
|
|
|
|
HSCT, yes |
0.39 (0.197−0.769; 0.007) |
0.69 (0.397−1.212; 0.198) |
1.05 (0.514−2.162; 0.886) |
|
Induction |
|
|
|
Safety
Compared with the SDC group, patients in the LDC group showed a significantly shorter period of neutrophil (median 20 vs 12 days, respectively; p < 0.001), and platelet recovery (median 16 vs 11 days, respectively; p < 0.001). Grade 3 or 4 febrile neutropenia was higher in SDC compared with the LDC group (91% vs 61%). The LDC group was more cost-effective and showed an overall cost of treatment for induction I and II lower than the SDC group ($6,279 vs $7,257, respectively; p = 0.01).
Gene mutations after induction I and II
The average variant allele frequency (VAF) after induction I decreased from 29.1% to 1.9% in the LDC group and from 29.1% to 0.6% in the SDC group (p < 0.001). A greater VAF decrease was observed after induction II, to 0.17% in LDC group, and 0.078% in the SDC group (p = 0.052).
Conclusion
The study confirmed that the induction responses, OS, EFS, and CIR were similar across both groups. The LDC group demonstrated an advantage of shorter periods of neutropenia and thrombocytopenia, reduced frequency of Grade 3 or 4 complications, and reduced overall cost compared with the SDC group. These findings suggest that in general, pediatric AML is highly sensitive to chemotherapy at diagnosis, and that the leukemia cell burden can be considerably reduced by adapting to low-dose myelosuppressive treatment approaches. These approaches also come with the benefit of a lower treatment burden. However, further evidence is needed on these approaches in LMICs.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?