All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Increased risk of NRM and its associated factors in patients with chronic GvHD: an updated analysis
Chronic graft-versus-host disease (cGvHD) is responsible for late morbidity, impaired quality of life, and is the main driver of non-relapse mortality (NRM) in patients after allogeneic hematopoietic stem cell transplantation (allo-HSCT). There is emerging evidence from a large US study of an increased incidence of cGvHD in patients between 1995 and 2007 (odds ratio, 1.19; p < 0.0001) over three intervals (1995–1999, 2000–2003, and 2004–2007). Although NRM rates decreased at 1 and 3 years, no significant difference was seen at 5 years post-transplant, suggesting outcomes for late NRM had not improved. In addition, it also remains unclear whether advances in the management of allo-HSCT and the expanding knowledge of the pathophysiology of cGvHD have led to a reduced risk of NRM.
Here we report the key findings from a recent study by DeFilipp et al.1 published in Blood Advances, seeking to determine the cumulative incidence of cGvHD and NRM, and patient-, transplant-, and cGvHD-related risk factors for NRM.
Study design
This was a cohort study comprising data collected from adult patients (≥18 years) enrolled at 15 US institutions between 2007 and 2019 from two prospective studies through the cGvHD Consortium. Eligible patients with cGvHD had received allo-HSCT requiring new or a change in systemic immunosuppressive therapy.
Enrolled patients with cGvHD were grouped into two categories: incident (<3 months after diagnosis) or prevalent (≥3 months but <3 years after diagnosis).
Provider-reported outcome data included the National Institute for Health (NIH) organ severity score of 0–3 for skin, eye, mouth, vulvovaginal, gastrointestinal, liver, lung, and joint. Patient-reported outcomes and functional measures included the Lee Symptom Scale, the Human Activity Profile (HAP), and the Short Form Health Survey (SF-36). The study also collected data on the year of transplantation, time from transplantation to cGvHD diagnosis, time from diagnosis to enrollment, incident versus prevalent cases, cause of death, and the parent clinical study.
Results
Baseline characteristics
A total of 937 patients were included; 60% of patients were male and the median age was 52 years (range, 18–78 years). The median year of transplantation was 2010 (range, 1987–2017). Most of the transplantations were performed for hematologic malignancies (95%), the most common conditioning regimen was myeloablative (51%), and the graft source was mostly peripheral blood (90%) (Table 1).
Table 1. Baseline characteristics*
|
ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; CLL, chronic lymphocytic leukemia; CML, chronic myeloid leukemia; GvHD, graft-versus-host disease; HL, Hodgkin lymphoma; MDS, myelodysplastic syndromes; MPD, myeloproliferative disorders; NHL, non-Hodgkin lymphoma; NMA, non-myeloablative; RIC, reduced-intensity conditioning. |
|||
|
Characteristic, % |
Total |
Alive |
Died |
|---|---|---|---|
|
Diagnosis |
|
|
|
|
AML/ALL |
47 |
47 |
47 |
|
CML/CLL |
11 |
11 |
12 |
|
MDS/MPD |
17 |
17 |
17 |
|
NHL/HL |
16 |
16 |
16 |
|
Donor type |
|
|
|
|
Matched related |
38 |
39 |
37 |
|
Matched unrelated |
47 |
46 |
48 |
|
Mismatched |
15 |
15 |
15 |
|
Graft source |
|
|
|
|
Peripheral blood |
90 |
89 |
91 |
|
Bone marrow |
6 |
7 |
5 |
|
Cord blood |
4 |
4 |
4 |
|
Conditioning intensity |
|
|
|
|
Myeloablative |
51 |
54 |
44 |
|
RIC/NMA |
49 |
46 |
56 |
|
Acute GvHD Grades II–IV |
50 |
48 |
54 |
|
Relapse |
15 |
6 |
32 |
cGvHD characteristics and patient-reported outcomes
The median time from transplantation to cGvHD diagnosis was 8 months (interquartile range, 7–23 months) and the median time from HSCT to cGvHD was 7.5 months (range, 1–141 months). At baseline, the NIH cGvHD severity scores were mild, moderate, and severe in 13%, 49%, and 37% of patients, respectively. The most common organs involved at enrolment included skin (68%), mouth (60%), and eyes (55%).
The occurrence of high-risk laboratory indicators such as platelet count <100 × 109/L or total bilirubin >2 mg/dL were rare (15% and 4%, respectively). During the study, minimal differences were observed in cGvHD and patient-reported outcomes between patients who died and those who survived. The frequency of an NIH severity score of 2–3 was low in all involved organs except skin (49%).
NRM and causes of death
A total of 333 deaths were reported; the median follow-up for survivors was 4 years (range, 0.1 months to 12.5 years) and relapse accounted for 25% of deaths. The cumulative incidence of NRM was 7% at 1 year (95% confidence interval [CI], 6–9%), 15% at 3 years (95% CI, 13–17%), 22% at 5 years (95% CI, 19–25%), and 40% at 12 years (95% CI, 30–50%).
The most common cause of NRM was cGvHD-associated organ failure, infection, or additional causes not otherwise specified. The next most common causes without mention of cGvHD included infection, respiratory failure, and non-respiratory organ failure (Figure 1). The cause of death was unknown in 23% of patients.
Figure 1. Primary causes of death for non-relapse mortality cases*
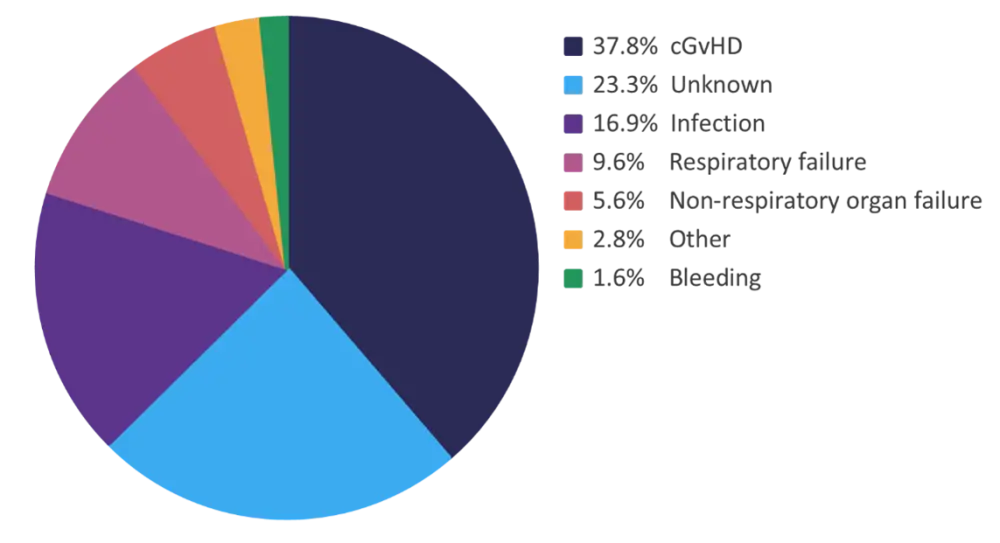
cGvHD, chronic graft-versus-host disease.
*Adapted from DeFilipp, et al.1
In multivariable analysis, an increased risk of NRM was significantly associated with reduced-intensity conditioning, total bilirubin >2 mg/dL, skin scores 2–3, lung score 1–3, worse modified HAP-adjusted activity score, and decreased distance on walk test (Table 2).
Table 2. Multivariable analysis of variables*
|
CI, confidence interval; HAP, human activity profile; HR, hazard ratio; RIC, reduced-intensity conditioning; NMA, non-myeloablative. |
||
|
Variable |
HR (95% CI) |
p value† |
|---|---|---|
|
Conditioning regimen |
|
|
|
RIC/NMA |
1.5 (1.1–2.1) |
0.024 |
|
Bilirubin at enrolment, mg/dL |
|
|
|
>2 |
2.24 (1.16–4.34) |
0.017 |
|
Skin score at enrolment |
|
|
|
0–1 |
1.21 (0.72–2.05) |
0.47 |
|
2–3 |
1.89 (1.27–2.82) |
0.002 |
|
Lung score at enrolment |
|
|
|
0–1 |
1.68 (1.14–2.49) |
0.009 |
|
2–3 |
2.25 (1.35–3.75) |
0.002 |
|
Walk test (per 10 feet) |
0.97 (0.96–0.99) |
0.001 |
|
Modified HAP-adjusted activity score (per 10 points) |
0.80 (0.70–1.0) |
0.012 |
Conclusion
This retrospective cohort study demonstrated that the risk of NRM does not plateau and continues to increase over time in patients with cGvHD. The increased risk of NRM was most attributed to GvHD or infection. High-risk biochemical features such as total bilirubin >2 mg/dL and skin and lung involvement (score 2–3) were identified to be associated with NRM. One of the strengths of this study was the inclusion of detailed cGvHD characteristics allowing evaluation of many more variables than have previously been investigated. The authors suggested that although reduced-intensity conditioning was associated with increased NRM, other factors such as older patient age, worse performance status, or increased comorbidities that were not independently associated with NRM may have contributed to this increased risk. The study was limited by a higher proportion of patients with moderate or severe disease due to the eligibility criteria and may not be representative of the whole cGvHD population. The data used were collected at the time of study entry and therefore are limited in identifying changes in cGvHD-related factors over time. The cause of death was reported by the participating centers with no specific guidelines to follow, with recording of cGvHD activity or contribution to death non-standard, which could have resulted in an underestimation of effect. In addition, the effect of systemic therapy was not evaluable, and the impact of novel approaches for the prevention and treatment of cGvHD on the risk of NRM were unknown. Advanced skin and lung cGvHD remain challenging indices associated with increased risk of NRM and further research on novel therapeutic options is warranted.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?