All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Impact on outcomes of non-T-depleted haplo-SCT and PTCy in patients with sAML vs de novo AML
Do you know... What is the main factor leading to patients with sAML being at increased risk of poorer outcomes and overall prognosis?
In comparison with de novo acute myeloid leukemia (AML), patients with secondary AML (sAML) typically present with poorer overall outcomes, including lower levels of complete remission (CR), relapse-free survival, and a reduced overall survival rate.1 These inferior outcomes in patients with sAML are attributable to an increased likelihood of adverse molecular mutations and high-risk cytogenetic abnormalities in addition to being older and having prior hematologic disease.
The AML Hub is pleased to summarize a recent study by Nagler et al.1 comparing the impact of non-T-depleted haploidentical hematopoietic stem cell transplantation (haplo-HSCT) in combination with posttransplant cyclophosphamide (PTCy) on clinical outcomes in patients with sAML versus de novo AML in first CR.
Study design1
This was a retrospective analysis from the Acute Leukemia Working Party (ALWP) of the European Society for Blood and Marrow Transplantation (EBMT) in patients aged ≥18 years with de novo or sAML in first CR who underwent a first HSCT between 2010 and 2021 from a haploidentical donor and were treated with PTCy. To validate the general population data and limit the impact of individual variables, a matched-pair analysis in a ratio of 1:2 (sAML: de novo AML) was also conducted. Table 1 outlines the baseline characteristics of both cohorts.
Table 1. Baseline patient characteristics*
|
AML, acute myeloid leukemia; CMV, cytomegalovirus; HCT-CI, hematopoietic cell transplantation specific comorbidity index; MRD, measurable residual disease; sAML, secondary AML. |
|||
|
Characteristic, % (unless otherwise stated) |
de novo AML cohort |
sAML cohort |
p value |
|---|---|---|---|
|
Median age (range), years |
55.8 |
60.8 |
<0.0001 |
|
Sex |
|
|
|
|
Male |
57.5 |
61.9 |
0.21 |
|
Female |
42.5 |
38.1 |
— |
|
Adverse cytogenetics |
29.9 |
32.9 |
— |
|
Median time from diagnosis to HSCT (range), months |
5.2 |
4.9 |
0.005 |
|
MRD pretransplant |
|||
|
Negative |
63.5 |
59.4 |
0.51 |
|
Positive |
36.5 |
40.6 |
— |
|
HCT-CI |
|
|
|
|
HCT-CI = 0 |
57.1 |
41.8 |
<0.0001 |
|
HCT-CI = 1 or 2 |
21.6 |
17.4 |
— |
|
HCT-CI ≥3 |
21.3 |
40.8 |
— |
|
Karnofsky score |
|||
|
<90 |
22.0 |
31.5 |
0.002 |
|
≥90 |
78.0 |
68.5 |
— |
|
Patient CMV |
|||
|
Negative |
21.3 |
23.8 |
0.4 |
|
Positive |
78.7 |
76.2 |
— |
|
Donor CMV |
|||
|
Negative |
37.3 |
43.8 |
0.063 |
|
Positive |
62.7 |
56.2 |
— |
Results1
Transplantation outcomes
Incidence of engraftment (95.1% vs 94.4%) and acute graft-versus-host disease (aGvHD) Grade 1–2 (27.2% vs 29.1%) and Grade 3–4 (9.2% vs 6.6%) did not differ significantly between sAML and de novo AML cohorts, respectively. The 2-year incidence of chronic GvHD was also similar between the sAML and de novo AML cohorts (32.2% vs 33.3%, respectively). The presence of prior hematologic disorders did not impact the transplant outcomes in either cohort; Table 2 shows sAML per antecedent hematologic disorder versus de novo AML for posttransplant outcomes.
Table 2. sAML per antecedent hematologic disorder versus de novo AML in posttransplant outcomes*
|
aGvHD, acute graft-versus-host disease; AML, acute myeloid leukemia; BMFS, bone marrow failure syndrome; cGvHD, chronic GvHD; GRFS, GvHD-free relapse-free survival; HR, hazard ratio; LFS, leukemia-free survival; MDS, myelodysplastic syndrome; MPN, myeloproliferative neoplasm; NRM, non-relapse mortality; OS, overall survival; OMHD/ST, other malignant hematologic disorders/solid tumors. |
|||
|
Relative risk, HR (p value) |
de novo AML |
MDS/MPN/BMFS |
OMHD/ST |
|---|---|---|---|
|
Relapse |
1 |
1.02 (0.91) |
1.01 (0.96) |
|
NRM |
1 |
0.87 (0.5) |
1.18 (0.52) |
|
LFS |
1 |
0.95 (0.73) |
1.1 (0.62) |
|
OS |
1 |
0.88 (0.43) |
1.1 (0.63) |
|
GRFS |
1 |
0.97 (0.8) |
0.89 (0.52) |
|
aGvHD II–IV |
1 |
1.09 (0.65) |
0.95 (0.84) |
|
aGvHD III–IV |
1 |
0.77 (0.47) |
0.66 (0.42) |
|
cGvHD |
1 |
1.14 (0.42) |
0.62 (0.099) |
|
Extensive cGvHD |
1 |
0.81 (0.46) |
0.32 (0.055) |
Leukemia-free survival, overall survival, non-relapse mortality, GvHD-free relapse-free survival, and relapse rates (Figure 1) were similar between patients with de novo and sAML.
Figure 1. 2-year posttransplant outcomes in the general population*
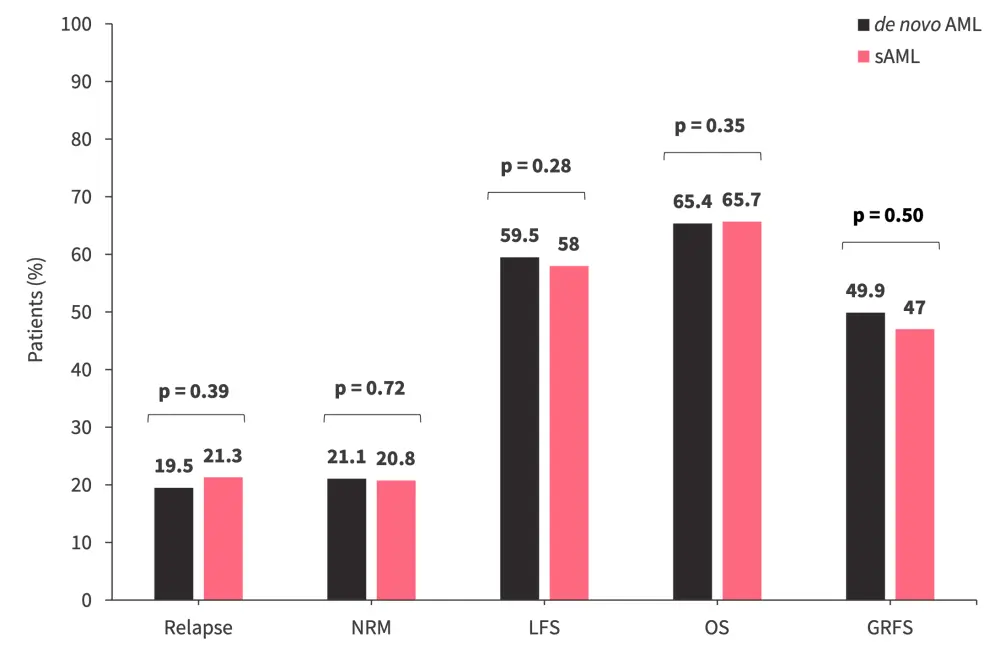
AML, acute myeloid leukemia; GRFS, GvHD-free relapse-free survival; GvHD, graft-versus-host disease; LFS, leukemia-free survival; NRM, non-relapse mortality; OS, overall survival; sAML secondary AML.
*Data from Nagler, et al.1
Matched-pair analysis
The findings from the matched-pair analysis were consistent with previously reported data, highlighting no significant difference in the outcomes of patients with de novo AML and sAML following haplo-HSCT and PTCy. Relapse rates were 21.4% in the de novo arm compared with 21% in the sAML arm. Figure 2 shows matched-pair data at 2 years posttransplant for corresponding clinical outcomes including relapse, non-relapse mortality, leukemia-free survival, overall survival, and GvHD-free relapse-free survival.
Figure 2. Matched-pair analysis of posttransplant outcomes in de novo and sAML cohorts*
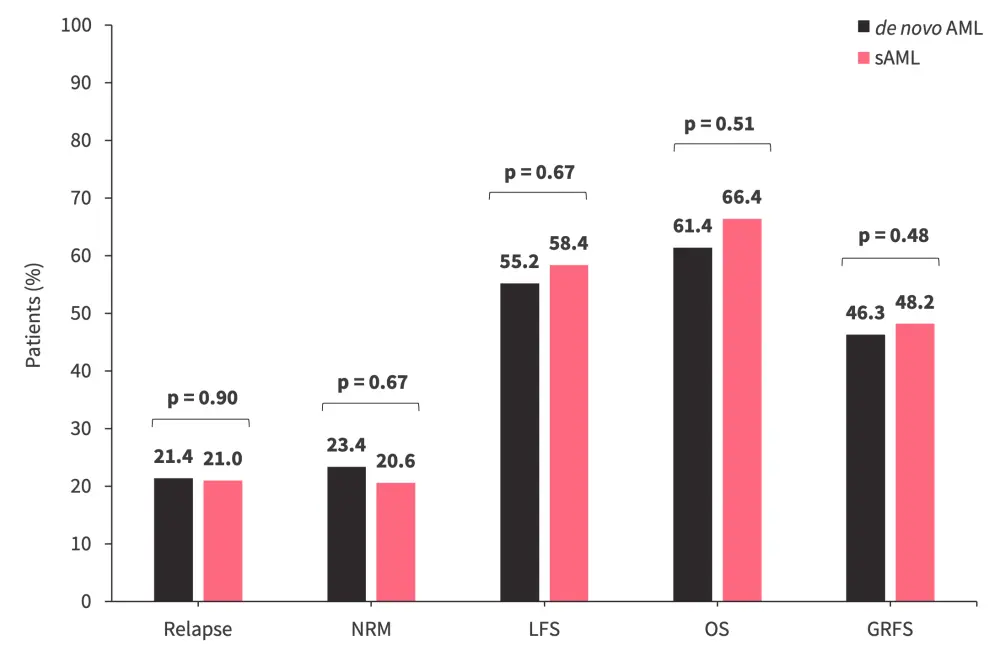
AML, acute myeloid leukemia; GRFS, GvHD-free relapse-free survival; GvHD, graft-versus-host disease; LFS, leukemia-free survival; NRM, non-relapse mortality; OS, overall survival; sAML secondary AML.
*Data from Nagler, et al.1
Mortality rates
During the study period, a total of 564 patients died, with the most common cause of death being the original disease. Infection-related mortality was the second most frequent cause, accounting for 30.5% and 26.3% of deaths in the de novo AML and sAML cohorts, respectively (Figure 3).
Figure 3. Causes of death in de novo and sAML cohorts*
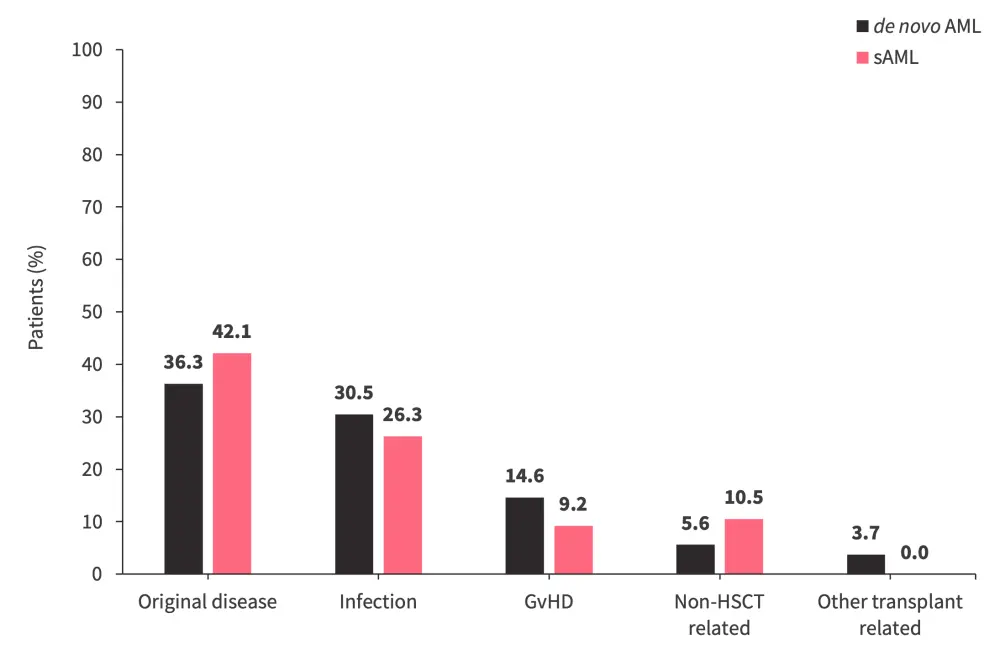
AML, acute myeloid leukemia; GvHD, graft-versus-host disease; HSCT, hematopoietic stem cell transplant; sAML, secondary AML.
*Data from Nagler, et al.1
Conclusion
This retrospective analysis demonstrates that transplantation outcomes were similar between de novo AML and sAML cohorts. In addition, there were no differences observed in the transplantation outcomes irrespective of prior hematologic disease. The findings suggest that haplo-HSCT in combination with PTCy may present a strategy to overcome the typically poor prognosis of patients with sAML. However, the findings were limited by the study design being retrospective in nature and limited to patients in CR1; therefore only presenting favorable outcome data for comparison.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?