All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
FLA-IDA with or without venetoclax in patients with relapsed/refractory acute myeloid leukemia
Do you know... Which of the following benefits would you expect to see in patients with relapsed/refractory AML treated with venetoclax and FLA-IDA (FLAVIDA) versus FLA-IDA monotherapy?
Venetoclax, a BCL-2 inhibitor that has been extensively covered by the AML Hub, may improve outcomes in patients with relapsed/refractory (R/R) acute myeloid leukemia (AML) when combined with intensive salvage chemotherapy.1
While the benefit of venetoclax in lower-intensity regimens has been demonstrated in AML treatment, as evidenced by results from the phase III VIALE-A trial (NCT02993523), there are several studies investigating how venetoclax can improve response rates in higher-intensity regimens.1 The AML Hub has previously covered a phase Ib/II (NCT03214562) and phase II trial (NCT02115295) evaluating the addition of venetoclax to FLAG-IDA (fludarabine, cytarabine, granulocyte colony-stimulating factor, and idarubicin) and cladribine with high-dose cytarabine and idarubicin, respectively, in patients with AML. These studies suggest that venetoclax plus intensive chemotherapy is associated with high response rates; however, it is not yet clear whether these response rates can be translated into improved survival outcomes.1
Recently, Shahswar et al.1 published a retrospective analysis in Haematologica assessing the addition of venetoclax to FLA-IDA (fludarabine, cytarabine, and idarubicin) as a salvage therapy for patients with R/R AML, which we are pleased to summarize below.
Study design1
This analysis included patients aged ≥18 years with R/R AML treated with FLA-IDA plus venetoclax (FLAVIDA) between May 2018 and July 2021. Patients received FLA-IDA plus 100 mg oral venetoclax once daily on Days 1–7. The control cohort comprised patients treated with FLA-IDA between 2000 and 2018 from the Hannover Medical School database.
The primary endpoints were the safety and tolerability of FLAVIDA and the overall response rate. Secondary endpoints included the measurable residual disease (MRD)-negative response rate and survival outcomes.
Baseline characteristics
In total, 37 and 81 sequentially treated patients were included in the FLAVIDA and FLA-IDA groups, respectively. Baseline characteristics were similar between the two groups (Table 1).
Table 1. Baseline characteristics*
|
AML, acute myeloid leukemia; CR, complete remission; FLA-IDA; fludarabine, cytarabine, and idarubicin; FLAVIDA, FLA-IDA + venetoclax; ELN, European LeukemiaNet; G-CSF, granulocyte colony-stimulating factor. |
||||
|
Characteristics, % (unless otherwise stated) |
FLAVIDA |
FLA-IDA |
p value |
|
|---|---|---|---|---|
|
Median age (range), years |
54 (19–70) |
52 (22–72) |
0.95 |
|
|
Sex |
|
|
0.9 |
|
|
Male |
57 |
56 |
||
|
Female |
43 |
44 |
||
|
Type of AML |
|
|
0.26 |
|
|
De novo |
70 |
77 |
||
|
Secondary |
27 |
19 |
||
|
Therapy-related |
3 |
5 |
||
|
ELN 2017 risk group |
|
|
0.26 |
|
|
Favorable |
16 |
25 |
||
|
Intermediate |
51 |
46 |
||
|
Adverse |
33 |
25 |
||
|
Missing |
0 |
5 |
||
|
Treatment lines before FLAVIDA |
|
|
0.91 |
|
|
Median (range), n |
1 (1–5) |
1 (1–4) |
||
|
Salvage 1 |
70 |
70 |
||
|
Salvage 2 |
25 |
20 |
||
|
Salvage ≥3 |
5 |
10 |
||
|
Disease status |
|
|
0.5 |
|
|
Refractory AML |
49 |
42 |
||
|
Relapsed AML |
51 |
58 |
||
|
Mutations† |
|
|
|
|
|
DNMT3A |
36 |
33 |
0.78 |
|
|
NPM1 |
31 |
22 |
0.36 |
|
|
SRSF2 |
25 |
5 |
<0.01 |
|
|
FLT3-ITD |
22 |
30 |
0.39 |
|
|
IDH1 |
6 |
6 |
0.66 |
|
|
IDH2 |
22 |
14 |
0.31 |
|
|
RUNX1 |
19 |
8 |
0.09 |
|
|
NF1 |
17 |
8 |
0.18 |
|
|
K/NRAS |
11 |
13 |
0.82 |
|
|
TP53 |
6 |
6 |
0.87 |
|
|
Use of G-CSF after FLAVIDA |
|
|
0.63 |
|
|
Yes |
68 |
69 |
||
|
No |
32 |
25 |
||
|
Missing |
0 |
6 |
||
Key findings1
Response
All patients received ≥1 cycle of FLAVIDA or FLA-IDA. When compared with the FLA-IDA group, treatment with FLAVIDA was associated with,
- a higher overall response rate (78% vs 47%; p = 0.001; Figure 1); and
- a higher composite complete remission rate (59% vs 30%; p = 0.003; Figure 1).
Data on MRD status following one treatment cycle was available for 26 and 23 patients with an overall response in the FLAVIDA and FLA-IDA groups, respectively. The proportion of MRD-negative (MRD−) response was similar between the two groups (FLAVIDA, 50%; FLA-IDA, 57%; p = 0.65).
Figure 1. Response rates in the FLAVIDA versus FLA-IDA groups *
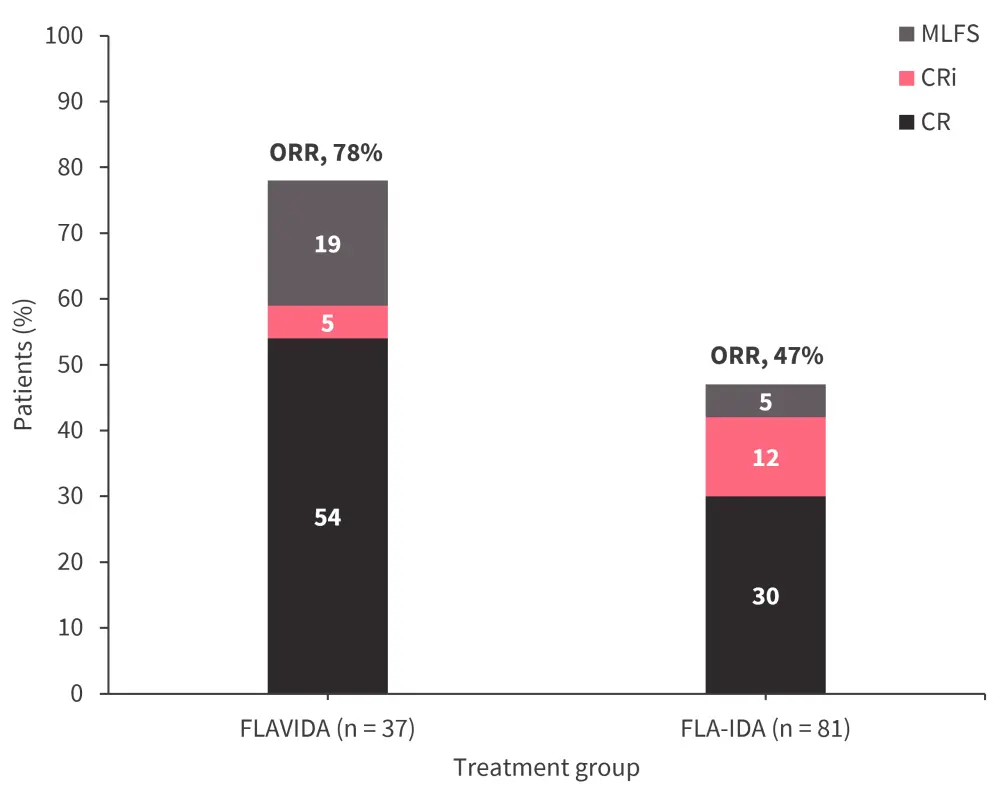
AML, acute myeloid leukemia; CI, confidence interval; CR, complete remission; CRi, CR with incomplete hematological recovery; FLA-IDA; fludarabine, cytarabine, and idarubicin; FLAVIDA, FLA-IDA + venetoclax; MLFS, morphologic leukemia-free state; OR, odds ratio; ORR, overall response rate; R/R, relapsed/refractory.
*Adapted from Shahswar, et al.1
Transplant
In the FLAVIDA group, 81% of patients proceeded to allogeneic hematopoietic stem cell transplantation (allo-HSCT; n = 27) or received donor lymphocyte infusions (n = 3). In the FLA-IDA group, 79% of patients proceeded to allo-HSCT (n = 49) or received donor lymphocyte infusions (n = 15).
Survival
The median follow-up was 22.4 months and 62.9 months in the FLAVIDA and FLA-IDA groups, respectively. While response rates were higher in the FLAVIDA group, this did not translate into improved survival outcomes:
- Overall survival (OS) was similar between treatment groups after propensity score weighting (hazard ratio [HR], 1.25; p = 0.4; Figure 2).
- Median event-free survival (EFS) was similar between the FLAVIDA and FLA-IDA groups (11.3 months vs 6.9 months; HR, 0.7; p = 0.1).
Subgroup analysis revealed an EFS benefit with FLAVIDA vs FLA-IDA in patients with IDH1/2 mutations (HR, 0.3; 95% confidence interval [CI], 0.11–0.85), while OS was similar between the two treatment groups in this patient group (HR, 0.81; 95% CI, 0.25–2.60). In patients who did not respond to treatment, FLAVIDA was associated with poorer EFS (HR, 1.80; 95% CI, 1.12–2.89) and OS (HR, 3.37; 95% CI, 1.26–8.99) when compared with FLA-IDA.
MRD data was available for 26 and 23 patients treated with FLAVIDA and FLA-IDA, respectively. MRD− patients treated with FLAVIDA had longer OS than MRD-positive patients (HR, 0.1; 95% CI, 0.01–0.59; p = 0.01). While the percentage of patients in the FLA-IDA group with MRD data available was low (28%), MRD was not prognostic for OS in responders (HR, 0.41; 95% CI, 0.1–1.7; p = 0.23). Among MRD− patients, the OS was similar between the FLAVIDA and FLA-IDA (p = 0.4; Figure 2).
Figure 2. 1- and 2-year OS rates*
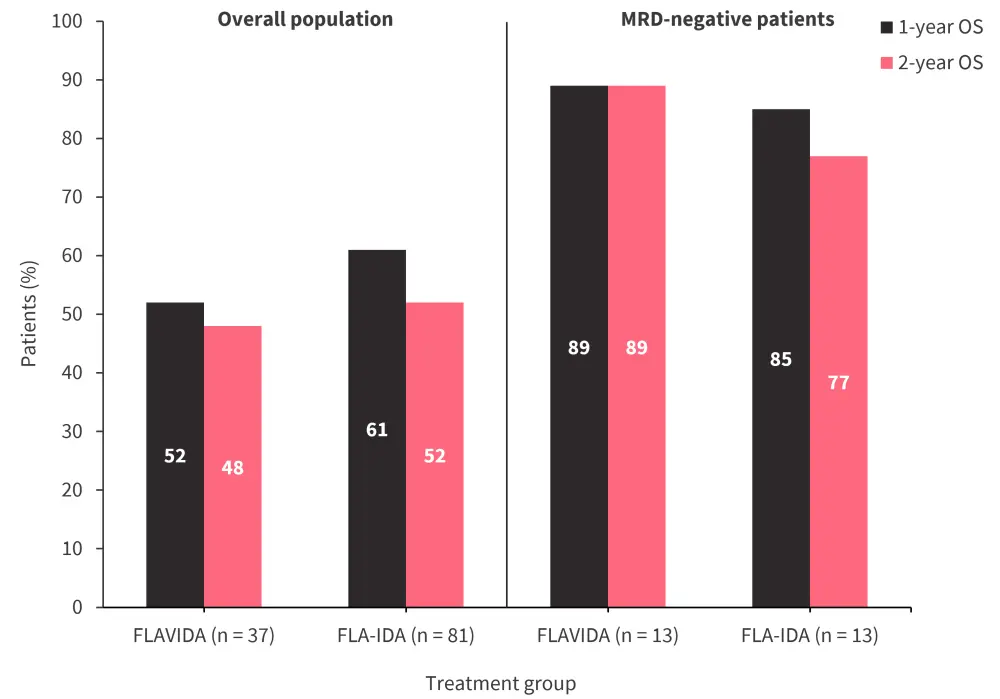
FLA-IDA; fludarabine, cytarabine, and idarubicin; FLAVIDA, FLA-IDA + venetoclax; OS, overall survival; MRD, measurable residual disease.
*Adapted from Shahswar, et al.1
Safety
One patient died within 30 days of initiating FLAVIDA treatment, this was due to multi-organ failure following pneumonia. Hematologic adverse events were the most commonly observed treatment-related toxicities, including anemia (100%), thrombocytopenia (100%), and febrile neutropenia (97%) (Table 2). The most common non-hematologic adverse events were bacteremia (27%), sepsis (11%), and fungal pneumonia (11%; Table 2). In responding FLAVIDA patients, the median time to neutrophil recovery (>500/nL) was 33 days (95% CI, 30–36), compared with 28 days (95% CI, 23–33) in FLA-IDA patients (p = 0.94). The median time for platelet recovery (>50/nL) was 35 days (95% CI, 32–38) in the FLAVIDA group and 34 days (95% CI, 27–41) in the FLA-IDA group (p = 0.85). Recovery time for platelet counts >100/nL for responding FLAVIDA patients was 36 days (95% CI, 33–39) versus 34 days (95% CI, 31–37) for FLA-IDA patients (p = 0.86).
Table 2. Treatment-emergent adverse events in the FLAVIDA group*
|
Treatment-emergent adverse events, % |
Any grade |
Grade 3/4 |
|---|---|---|
|
FLAVIDA, fludarabine, cytarabine, and idarubicin plus venetoclax. |
||
|
Anemia |
100 |
100 |
|
Thrombocytopenia |
100 |
100 |
|
Febrile neutropenia |
97 |
97 |
|
Bacteremia |
27 |
27 |
|
Sepsis |
11 |
11 |
|
Fungal pneumonia |
11 |
11 |
|
Viral infection |
11 |
0 |
|
Elevated liver enzymes |
11 |
11 |
|
Creatinine increased |
11 |
3 |
|
Nausea, vomiting |
8 |
0 |
|
Bleeding (vaginal, gastrointestinal, pulmonary) |
8 |
0 |
|
Infusion reaction |
5 |
0 |
|
Pneumonia |
3 |
3 |
|
Respiratory insufficiency |
3 |
3 |
|
Skin and soft tissue infections |
3 |
0 |
|
Urinary tract infection |
3 |
0 |
|
Cardiac disorder |
3 |
0 |
Conclusion
In this retrospective analysis, FLAVIDA was associated with improved response rates compared with FLA-IDA in patients with R/R AML. The data demonstrates FLAVIDA as an effective salvage therapy treatment option, particularly as a bridge to allo-HSCT. However, the higher response rate in the FLAVIDA group did not translate to improved survival outcomes versus FLA-IDA; the only exception was patients with IDH1/2 mutations, who showed improved EFS.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?

