All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Editorial theme | Transplant outcomes across AML mutational subgroups
Do you know... Which of the following mutations would you expect to confer a survival benefit after allo-HSCT?
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) can be curative for fit patients with acute myeloid leukemia (AML) through its graft-versus-leukemia effect.1 With increased donor availability and reduced-intensity conditioning regimens, allo-HSCT has become more accessible.1
As part of our editorial theme looking at transplant outcomes across AML patient populations, we are pleased to summarize a study by Kunadt et al.,2 published in the Journal of Hematology & Oncology, evaluating the impact of isocitrate dehydrogenase (IDH)1/2 mutations on allo-HSCT. Mutations in IDH genes occur in 15–20% of patients with AML. However, more information is needed on the prognosis associated with IDH mutations, with outcomes of allo-HSCT in patients with IDH mutations (IDHmut) limited to smaller studies.2
We also describe a study by Song et al.,3 published in Nature, assessing the effect of secondary-type mutations (STMs) on allo-HSCT. Mutations such as SRSF2, SF3B1, U2AF1, ZRSR2, ASXL1, EZH2, BCOR, and STAG2 are referred to as STMs due to their strong association with secondary AML. Generally, STMs confer an adverse prognosis; however, their impact on outcomes of patients undergoing allo-HSCT is not well understood.3
Impact of IDH1/2 mutations2
Study design and patient characteristics
This study analyzed 3,234 patients with AML aged <70 years who received allo-HSCT (n = 852) or consolidation chemotherapy (n = 2,382) in first complete remission (CR) (Figure 1). Patients were enrolled in the Study Alliance Leukemia (SAL) registry or one of the AML96, AML2003, AMLCG1999, AML60+, AMLCG2008, or SORAML clinical trials, and did not receive IDH1 or IDH2 inhibitors as part of their treatment. Bone marrow and peripheral blood samples were screened using denaturing high-performance liquid chromatography and analyzed by Sanger sequencing or next-generation sequencing.
Figure 1. Study design*
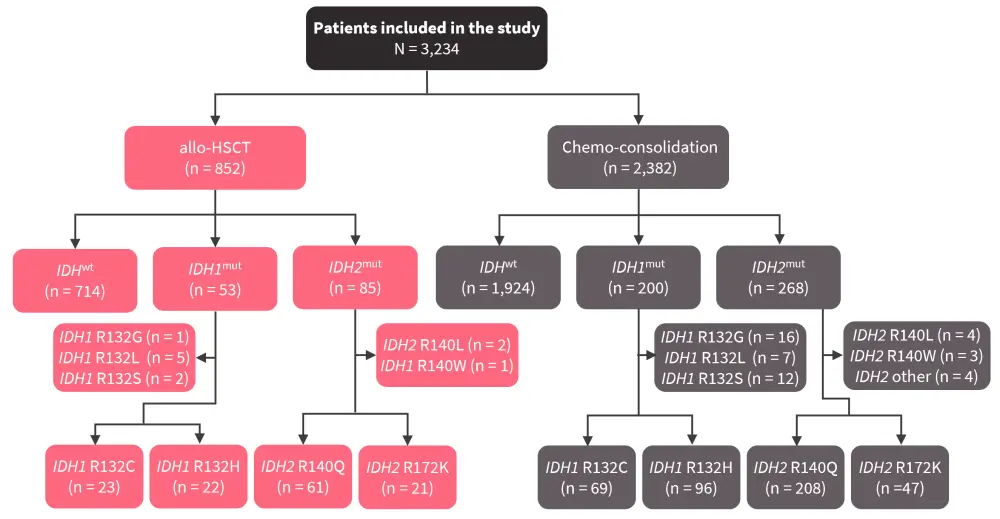
Allo-HSCT, allogeneic hematopoietic stem cell transplantation; IDH1/2mut, IDH1/2 mutation; IDHwt, IDH wild-type.
*Adapted from Kunadt, et al.2
In total, 18.4% of patients had mutations in IDH (IDHmut); 7.8% in IDH1 (IDH1mut), 10.9% in IDH2 (IDH2mut), and 0.3% in both IDH1/IDH2. The frequency of IDH1mut was lower in patients who received allo-HSCT compared with those who received consolidation chemotherapy (p = 0.042), whereas the frequency of IDH2mut was similar between treatment groups (p = 0.306).
The majority of patients harbored co-mutations
The majority of patients carried at least two different mutations (Table 1). Co-mutations in NPM1 were more common in IDHmut compared with IDH wild-type (IDHwt). Furthermore, mutations in NRAS and biallelic mutation in CEBPA were less frequent in patients with IDHmut compared with IDHwt. Mutations in WT1, DNMT3A, and TET2 were also significantly different between IDH groups. However, FLT3-ITD mutations were not significantly different between patients with IDHmut and IDHwt.
Table 1. Co-mutations of significance*
|
IDH1/2mut, IDH 1/2 mutations; IDHwt, IDH wild-type. |
||||
|
Co-mutation, % |
IDHwt |
IDH1mut |
IDH2mut |
p value |
|---|---|---|---|---|
|
ASXL1 |
3.9 |
4.3 |
7.8 |
0.059 |
|
BCOR |
2.5 |
2.6 |
4.4 |
0.342 |
|
BCORL1 |
2.2 |
2.6 |
3.9 |
0.383 |
|
CBL |
1.2 |
1.7 |
1.7 |
0.779 |
|
CEBPA biallelic |
6.4 |
0.5 |
1.1 |
<0.001 |
|
CSF3R |
1.1 |
1.7 |
1.1 |
0.825 |
|
CUX1 |
1.9 |
1.7 |
1.1 |
0.779 |
|
DNMT3A |
17.4 |
26.1 |
32.8 |
<0.001 |
|
EZH2 |
2.4 |
4.3 |
2.8 |
0.472 |
|
GATA2 |
6.5 |
0.9 |
2.2 |
0.005 |
|
IKZF1 |
1.6 |
1.7 |
0.6 |
0.543 |
|
JAK2 |
0.8 |
0.0 |
1.1 |
0.560 |
|
KDM6A |
0.4 |
1.7 |
0.0 |
0.089 |
|
KIT |
4.5 |
2.6 |
1.1 |
0.066 |
|
KRAS |
4.0 |
0.9 |
1.7 |
0.075 |
|
NPM1 |
32 |
59.1 |
45.3 |
<0.001 |
|
NRAS |
12.3 |
6.1 |
5.6 |
0.006 |
|
PHF6 |
1.9 |
0.9 |
1.1 |
0.553 |
|
PTPN11 |
4.5 |
5.2 |
3.3 |
0.711 |
|
RAD21 |
3.1 |
0.0 |
2.2 |
0.134 |
|
RUNX1 |
5.1 |
3.5 |
5.6 |
0.702 |
|
SMC1A |
1.2 |
0.9 |
0.0 |
0.955 |
|
SMC3 |
0.7 |
1.7 |
0.6 |
0.425 |
|
STAG2 |
2.9 |
4.3 |
6.7 |
0.029 |
|
TET2 |
12.4 |
3.5 |
7.2 |
0.003 |
|
TP53 |
3.0 |
0.9 |
0.6 |
0.072 |
|
WT1 |
7.0 |
1.7 |
2.2 |
0.006 |
|
ZRSR2 |
1.1 |
0.0 |
1.7 |
0.399 |
|
No co-mutations |
3.5 |
0.9 |
0 |
0.012 |
Survival outcomes by IDH mutational subgroup
A clinical benefit was detected in patients receiving allo-HSCT when compared with consolidation chemotherapy in IDHwt and IDHmut subgroups for overall survival (OS; hazard ratio [HR], 0.8; 95% confidence interval [CI], 0.69‑0.96; p = 0.012) and relapse-free survival (RFS; HR, 0.6; 95% CI, 0.54‑0.73; p < 0.001).
- Median OS and RFS were improved by allo-HSCT (Figure 2).
- Among patients who received allo-HSCT, patients with IDHmut tended to have longer survival compared to IDHwt.
- Conversely, among patients who received consolidation chemotherapy, patients with IDHmut tended to have shorter overall survival than patients with IDHwt.
- In patients with IDH1mut, 5-year OS was similar between treatment groups, whereas 5-year RFS was improved by allo-HSCT vs consolidation chemotherapy (51% vs 30%; p = 0.009).
- For patients with IDH2mut, allo-HSCT improved 5-year OS (61% vs 46%; p = 0.026), and RFS (60% vs 30%; p = 0.004), vs consolidation chemotherapy.
Figure 2. Survival outcomes by treatment type and IDH mutational status*
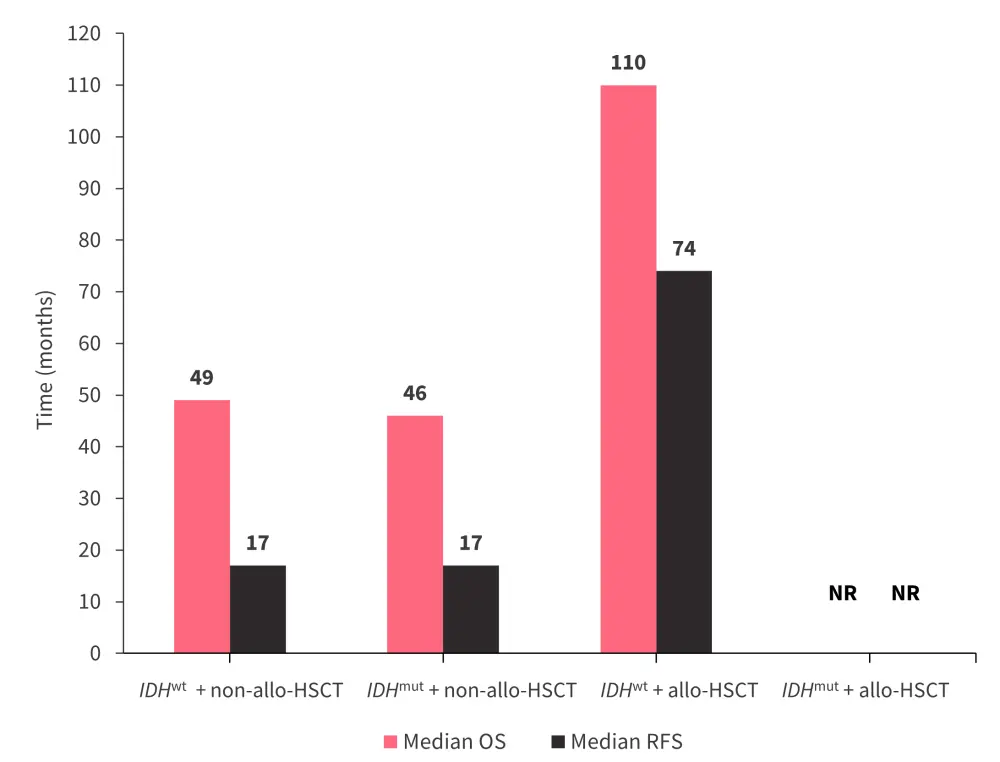
Allo-HSCT, allogeneic hematopoietic stem cell transplantation; IDHmut, IDH mutation; IDHwt, IDH wild-type; NR, not reached; OS, overall survival; RFS, relapse-free survival.
*Data from Kunadt, et al.2
Mutational subtype analysis revealed:
- Patients in the IDH1 R132C mutational subgroup who received allo-HSCT showed significant improvements in 5-year OS versus those who received consolidation chemotherapy (73% vs 40%; p = 0.017) and 5-year RFS (55% vs 27%; p = 0.048).
- IDH1 R132H mutations were not associated with superior survival.
- In patients with IDH2 R140, OS was similar between treatment groups, but 5-year RFS was improved with allo-HSCT versus consolidation chemotherapy (58% vs 31%; p = 0.002).
- In patients with IDH2 R172, allo-HSCT was associated with improved 5-year OS (68% vs 43%; p = 0.049) and RFS (64% vs 25%; p = 0.009) versus consolidation chemotherapy.
Multivariable and interaction analysis
In the multivariable analysis, OS and RFS were both influenced by age, favorable risk group, adverse risk groups, and the European LeukemiaNet risk categories and Eastern Cooperative Oncology Group performance status 0–1 (Table 2).
Table 2. Multivariable analysis*
|
ELN, European LeukemiaNet; ECOG, Eastern Cooperative Oncology Group; OS, overall survival; RFS, relapse-free survival. |
||||
|
Variable |
OS |
RFS |
||
|---|---|---|---|---|
|
HR |
p value |
HR |
p value |
|
|
Age |
1.03 |
<0.001 |
1.02 |
0.001 |
|
Favorable risk group |
0.6 |
<0.001 |
0.6 |
<0.001 |
|
Adverse risk group |
1.7 |
<0.001 |
1.5 |
0.001 |
|
ELN risk categories and ECOG performance status 0-1 |
0.7 |
0.00 |
0.8 |
0.001 |
Within the IDH mutational subgroups, IDH2 R172 was associated with better OS (HR, 0.5; p = 0.02) and RFS (HR, 0.4; p < 0.001). Interaction analysis was performed using allo-HSCT and IDHwt as reference terms. The effect of the interaction of IDHwt and consolidation chemotherapy, and the interaction of IDHmut subgroups and consolidation chemotherapy, predicted significantly worse survival outcomes:
- IDHwt
- OS: HR, 1.25; p = 0.006; and RFS; HR, 1.61; p < 0.001
- IDH1 R132H
- RFS: HR, 1.68; p = 0.008
- IDH2 R140Q
- OS: HR, 1.43; p = 0.023; and RFS: HR, 2.02; p < 0.001
- Other IDH mutational subgroups
- RFS: HR, 1.74; p = 0.043
Impact of STMs3
Study design and patient characteristics
This analysis included 394 patients aged >18 years with de novo AML and normal karyotype, diagnosed between 1998 and 2014. Patients were treated with an induction chemotherapy regimen, including a 3-day course of anthracyclines with a 7-day course of cytosine arabinoside or N4‑behenoyl-1-b-d-arabinofuranosylcytosine. Patients achieving CR received either allo-HSCT or consolidation chemotherapy. Patients received myeloablative (total body irradiation ≥8 Gy, oral busulfan ≥9 mg/kg, or intravenous busulfan ≥7.2 mg/kg) or reduced-intensity conditioning regimens. Cryopreserved bone marrow or peripheral blood samples were screened using next-generation sequencing.
Following genetic analysis, STMs were detected in 59 patients. Patients with STMs had a higher median age (p = 0.003) and were more likely to be male (p = 0.005) than patients without STMs. In total, 67.8% of patients with STMs and 87.5% of patients without STMs achieved CR. Of the patients with STMs who achieved CR, 25 received consolidation chemotherapy, and 15 received allo-HSCT. In patients without STMs who achieved CR, 166 received consolidation chemotherapy, and 127 received allo-HSCT.
EZH2 was the most common STM
- Among the patients with STMs, STMs occurred at the following frequencies: EZH2, 22.0%; SRSF2, 20.3%; U2AF1, 20.3%; BCOR, 18.6%; SF3B1, 15.3%, STAG2, 15.3%.
- CEBPA, FLT3-TKD, IDH1, and IDH2 mutations were detected at similar frequencies between patients with and without STMs.
- In the patients without STMs, NPM1 mutations (35.7% vs 22.0%; p = 0.043), FLT3-ITD mutations (23.1% vs 8.5%; p = 0.024), and DNMT3A mutations (25.8% vs 11.9%; p = 0.020) were more common than in patients with STMs.
- KRAS mutations were enriched in the patients with STMs (13.6% vs 3.3%; p = 0.003) when compared with patients without STMs.
Survival outcomes by STM status
The median follow-up was 80.1 months. Compared with patients without STMs, patients with STMs had:
- Lower CR rates (67.8% vs 87.5%; p < 0.001)
- Shorter 5-year OS (15.3% vs 31.0%; p < 0.001)
- Lower 5-year RFS among patients who achieved CR (20.0% vs 31.1%; p = 0.026)
- A trend towards higher non-relapse mortality and cumulative incidence of relapse (CIR), although these were not statistically significant
- Worse prognosis across age, sex, European LeukemiaNet risk stratification, and mutational subgroups
Analysis of patients according to treatment received found that those treated with consolidation chemotherapy and who harbored STMs had worse 5-year OS (12.0 vs 21.7%; p = 0.049) than those without, although RFS, CIR, and non-relapse mortality were similar. Furthermore, patients with STMs who received allo-HSCT had increased OS, and lower CIR, than patients with STMs who only received consolidation chemotherapy (Figure 3).
Figure 3. Outcomes in patients who achieved CR with STMs according to progression to allo-HSCT*
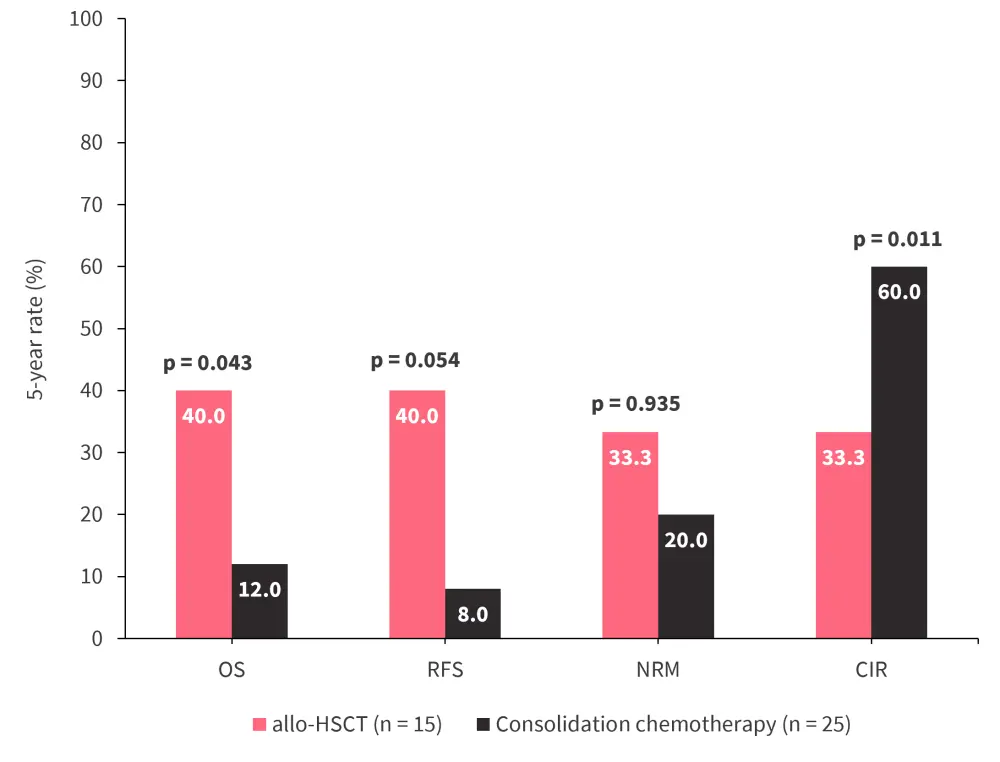
Allo-HSCT, allogeneic hematopoietic stem cell transplantation; CIR, cumulative incidence of relapse; CR, complete remission; NRM, non-relapse mortality; OS, overall survival; RFS, relapse-free survival.
*Data from Song, et al.3
Conclusion
In the study by Kunadt et al.2, allo-HSCT was shown to be beneficial in patients with IDHmut. However, results varied depending on mutational subgroups, with patients with IDH1 R132C and IDH2 R172 mutation showing the greatest improvement in survival outcomes as a result of receiving allo-HSCT. This study was limited by its retrospective nature and lack of donor information, patient performance status post-induction, and small patient numbers. Based on these results, further experimentation is warranted to define the impact of these mutational subgroups on allo-HSCT outcomes, and their prognostic relevance.
In the study by Song et al.3, the presence of STMs was associated with poorer clinical outcomes. Among patients with STMs, allo-HSCT conferred a survival benefit when compared with treatment with consolidation chemotherapy alone. The retrospective nature of the study was a limitation, along with the diverse types of conditioning regimens used, and the relatively small number of patients with STMs who received allo-HSCT. The genetic analysis also did not include the STM ZRSR2. However, a significant benefit of transplantation in patients with STMs was found.
Both studies demonstrated the prognostic value of the respective mutations assessed, the benefit of allo-HSCT in these patient groups, and the need for further investigation to confirm the impact of these mutations on transplant outcomes.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?
