All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Kura Oncology, Syndax, Abbvie, Thermo Fisher and Johnson & Johnson. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View AML content recommended for you
Allo-HSCT vs consolidation therapy to improve leukemia-free survival in elderly patients with AML
A significant proportion of older patients with acute myeloid leukemia (AML) will relapse after conventional treatment. Allogeneic hematopoietic stem cell transplantation (allo-HSCT) has been shown to reduce the risk of relapse and is being increasingly used in older patients. To date, randomized studies investigating allo-HSCT in elderly patients remain limited.
During the 50th Annual Meeting of the European Society for Blood and Marrow Transplantation, Niederwieser presented results from a randomized phase III study (NCT00766779) investigating whether allo-HSCT improves leukemia-free survival (LFS) vs non-allo-HSCT consolidation therapy in elderly patients with AML. We summarize this presentation below.
Study design1
-
Patients aged ≥60 and ≤75 years with AML were randomized 2:1 to receive fludarabine/total body irradiation plus cyclosporine/mycophenolate mofetil followed by allo-HSCT or non-allo-HSCT consolidation therapy.
-
The primary endpoint was LFS
-
-
Restricted mean survival time was used to compare LFS
-
-
Secondary endpoints were cumulative incidence (CI) of relapse, non-relapse mortality, and overall survival.
Key findings1
-
125 patients were randomized; however, only 66 proceeded to allo-HSCT and 35 completed the full consolidation regimen.
-
The primary endpoint of LFS was higher for patients treated with allo-HSCT vs those who were not (Figure 1).
-
There was a significant difference of 8.9 months in the restricted mean LFS associated with allo-HSCT vs non-allo-HSCT (p = 0.02).
Figure 1. Survival endpoints for elderly patients treated with allo-HSCT vs non-allo-HSCT consolidation therapy*
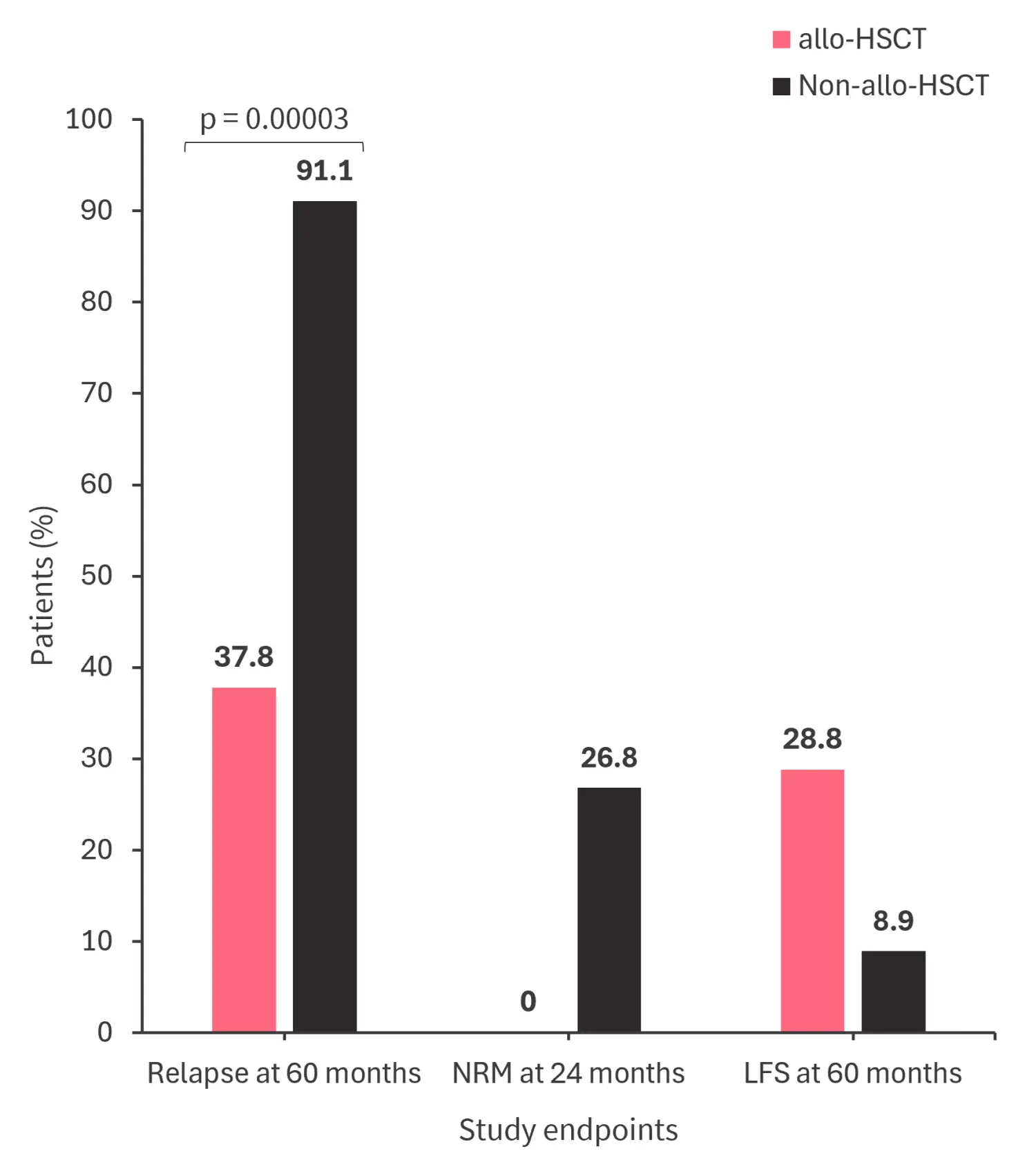
Allo-HSCT, allogeneic hematopoietic stem cell transplantation; LFS, leukemia-free survival; NRM, non-relapse mortality.
*Adapted from Niederwieser.1
- Overall survival was not statistically significant between the two study arms.
-
The CI of Grade 2–4 acute graft vs host disease was 31.8%.
-
The CI of limited and extensive chronic graft versus host disease was 45.5% and 33.5%, respectively.
-
The main cause of death in the allo-HSCT and non-allo-HSCT groups was relapse (50.9% vs 100%).
|
Key learnings |
|
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
What is the typical turnaround time for next-generation sequencing (NGS) results for AML at your center?