All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit Know AML.
The AML Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the AML Hub cannot guarantee the accuracy of translated content. The AML Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The AML Hub is an independent medical education platform, sponsored by Daiichi Sankyo, Johnson & Johnson, Syndax, Thermo Fisher Scientific, Kura Oncology, and AbbVie. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View AML content recommended for you
Allo-HSCT vs consolidation chemotherapy in younger patients with intermediate-risk AML
Do you know... Which subgroup of patients is likely to have a disease-free survival (DFS) benefit from allo-HSCT vs consolidation chemotherapy?
The optimal selection of patients with acute myeloid leukemia (AML) for allogeneic hematopoietic stem cell transplantation (allo-HSCT) is an area of research that continues to evolve.1 For patients with favorable-risk AML who achieve first complete remission (CR), there is a clear benefit associated with high-dose cytarabine-based consolidation chemotherapy, whereas patients with high-risk AML with adequate performance status and a suitable donor are candidates for allo-HSCT.
However, while allo-HSCT may be associated with lower rates of relapse in patients with intermediate-risk AML, there is an increased risk of transplant-related mortality. Moreover, at present, there is no agreed optimal treatment strategy for patients classified as intermediate risk; therefore, there is a need to explore the most beneficial therapy for this patient group.1
Here, we summarize the key points from the ETAL-1 trial by Bornhäuser et al.1 published in JAMA Oncology, evaluating allo-HSCT versus standard consolidation chemotherapy in patients with intermediate-risk AML.
Study design and patient characteristics
This was a phase III, prospective, randomized controlled trial (NCT01246752) conducted across 16 centers in Germany from 2011–2018. Eligible patients were aged 18–60 years with intermediate-risk AML in first CR or CR with incomplete hematological recovery, with a human leukocyte antigen-matched sibling or unrelated donor available. Patients were randomized 1:1 either to allo-HSCT or consolidation chemotherapy group according to:
- Age (18–40 years vs 41–60 years),
- NPM1 and CEBPA variant status
- Donor type (unrelated vs related)
In the consolidation chemotherapy group, patients who experienced hematologic or molecular relapse could subsequently receive allo-HSCT.
The primary endpoint was overall survival (OS). Secondary endpoints included disease-free survival (DFS), cumulative incidence of relapse (CIR), treatment-related mortality, and quality of life measured according to the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36) and safety.
In total, 76 patients were randomized to receive allo-HSCT and 67 patients to consolidation chemotherapy (Table 1).
Table 1. Patient characteristics*
|
Characteristics, % (unless otherwise stated) |
Allo-HSCT |
Consolidation chemotherapy |
|---|---|---|
|
Median age (range), years |
50.5 (19.0–60.0) |
51.0 (24.0–60.0) |
|
Age group |
|
|
|
18–40 years |
21 |
16 |
|
41–60 years |
79 |
84 |
|
CEBPA status |
|
|
|
Biallelic variant |
5 |
1 |
|
NPM1 status/FLT3-ITD status |
|
|
|
Variant/variant |
17 |
20 |
|
Variant/wild-type |
25 |
22 |
|
Wild-type/variant |
7 |
5 |
|
Wild-type/wild-type |
51 |
53 |
|
Missing |
9 |
4 |
|
ELN 2017 category |
|
|
|
Favorable |
32 |
28 |
|
Intermediate |
66 |
69 |
|
Adverse |
2 |
3 |
|
Available donor |
|
|
|
Matched sibling |
24 |
34 |
|
Matched unrelated (10/10) |
67 |
52 |
|
Mismatched unrelated (9/10) |
9 |
13 |
|
Allo-HSCT, allogeneic hematopoietic stem cell transplantation; ELN, European Leukemia Network; ITD, internal tandem duplication. |
||
Key points
Survival outcomes
- The 2-year OS rate was similar between the two groups (Figure 1).
- The 2-year DFS rate was higher in the allo-HSCT group compared with the consolidation chemotherapy group (Figure 1).
Figure 1. Survival outcomes by treatment group*
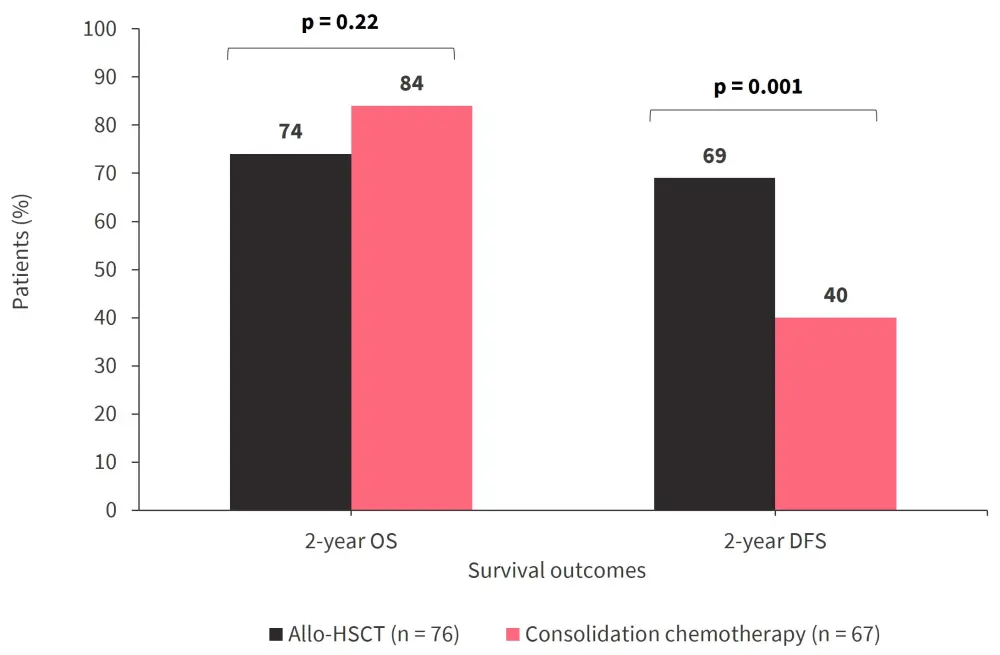
Allo-HSCT, allogeneic hematopoietic stem cell transplantation; DFS, disease-free survival; OS, overall survival.
*Data from Bornhäuser, et al.1
- Predefined subgroup analysis revealed that patients in the allo-HSCT group with non-favorable-risk AML, compatible unrelated donors, aged ≤40 years and >40 years, or who were male, had improved DFS compared with those in the consolidation chemotherapy group (Figure 2).
- Similar OS was also observed between the treatment groups (Figure 2).
Figure 2. The A OS and B DFS outcomes in patients treated with allo-HSCT versus consolidation chemotherapy by subgroup*
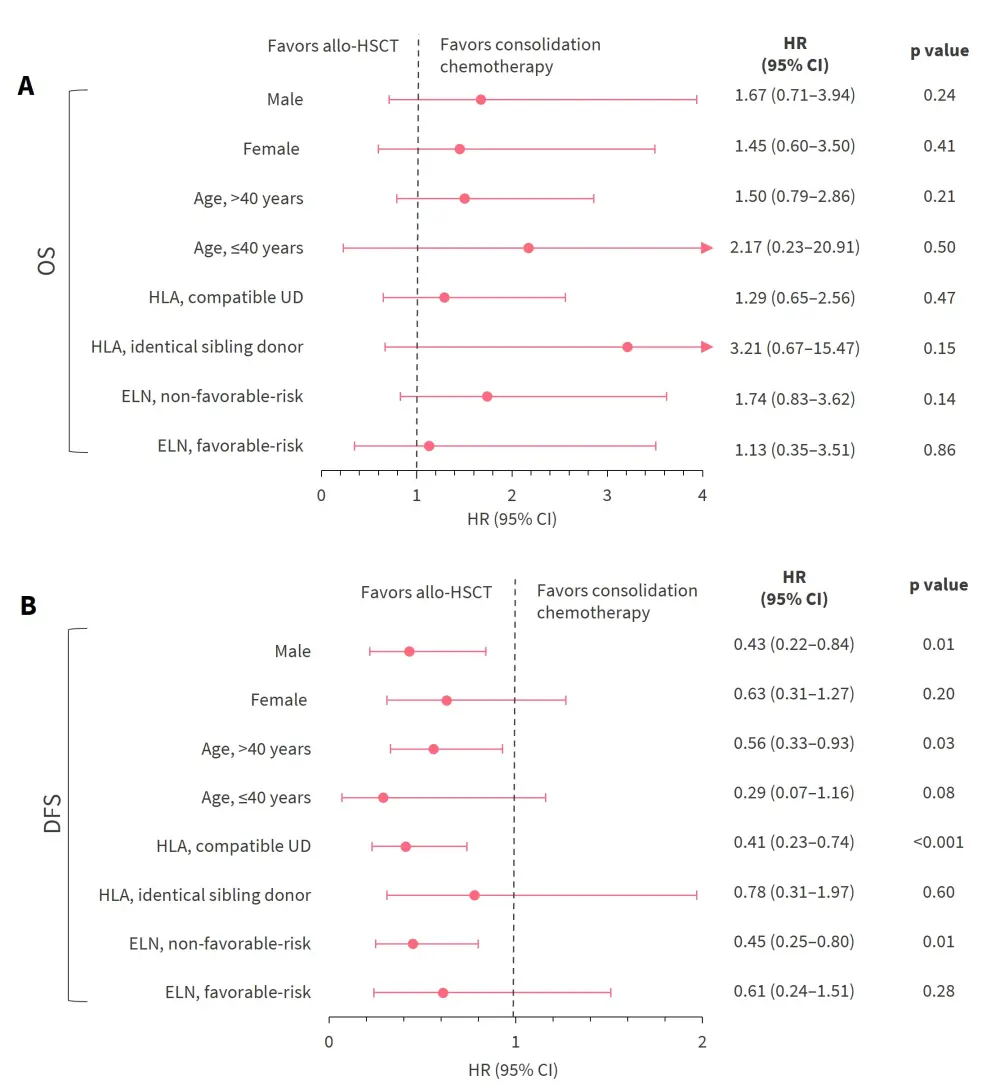
Allo-HSCT, allogeneic hematopoietic stem cell transplantation; CI, confidence interval; DFS, disease-free survival; ELN, European Leukemia Network; HLA, human leukocyte antigen; HR, hazard ratio; OS, overall survival; UD, unrelated donor.
*Adapted from Bornhäuser, et al.1
- Post hoc analysis of patients with intermediate-risk AML showed:
- No OS advantage in the allo-HSCT group compared with the consolidation chemotherapy group at 2 years (76% vs 83%, respectively).
- 2-year DFS rates were higher in the allo-HSCT group than the consolidation chemotherapy group (70% vs 39%; p = 0.02).
Non-relapse mortality, relapse incidence, and safety
- Allo-HSCT was associated with higher rates of 2-year non-relapse mortality but lower 2-year CIR compared with consolidation chemotherapy (Figure 3).
Figure 3. 2-year NRM and CIR by treatment group*
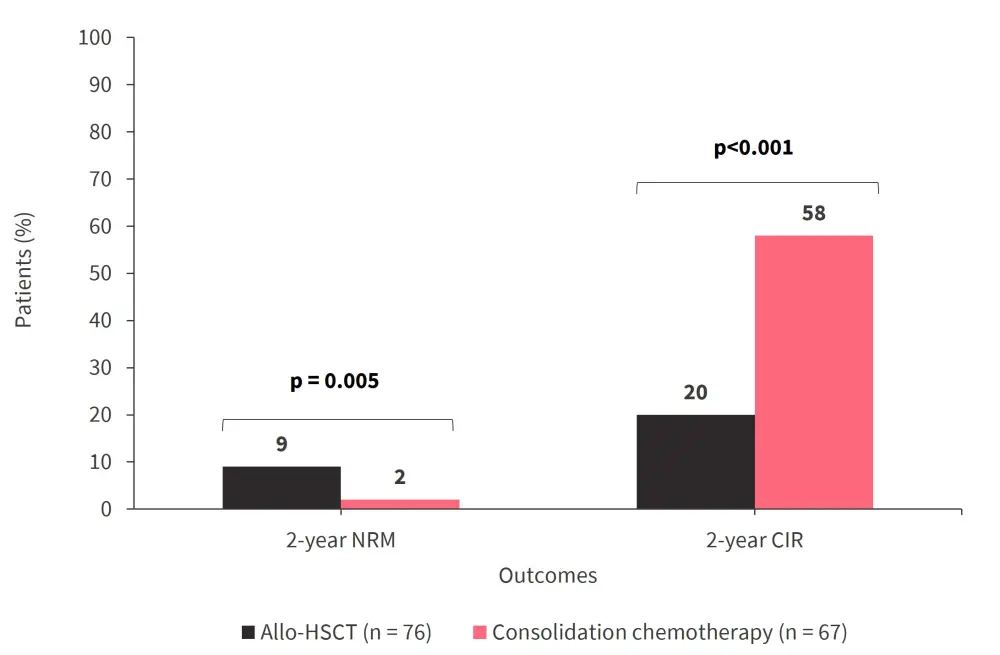
Allo-HSCT, allogeneic hematopoietic stem cell transplantation; CIR, cumulative incidences of relapse; NRM, non-relapse mortality.
*Data from Bornhäuser, et al.1
- All 41 patients in the consolidation chemotherapy group who relapsed received allo-HSCT either directly (n = 20) or after salvage therapy (n = 21).
- Incidences of serious adverse events were similar between the allo-HSCT group (74%) and the consolidation chemotherapy group (74%).
Quality of life outcomes
- The SF-36 scales were similar between the treatment groups.
- Patients in the allo-HSCT group had a shorter median duration of in-hospital stay (median, 42.5 days; interquartile range, 31.0–62.0) than patients in the consolidation chemotherapy group (median, 106.0 days; interquartile range, 72.0–143.0; p < 0.001).
Conclusion
While allo-HSCT was associated with improved DFS, this did not translate to an OS benefit in patients aged <60 years with intermediate-risk AML. Patients in the consolidation chemotherapy group who already had suitable donors identified were able to receive allo-HSCT either directly or after salvage therapy. Given the results of this study, younger patients with intermediate-risk AML may benefit from consolidation chemotherapy with measurable residual disease monitoring to detect early signs of potential relapse in patients for whom allo-HSCT may be beneficial. Further studies that apply longitudinal monitoring of measurable residual disease to optimize the timing of allo-HSCT for patients are warranted.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
Which AML-related topic do you currently need the most practical guidance on?